

Perioperative and Long-Term Outcomes in Patients Undergoing Synchronous Carotid Endarterectomy and Coronary Artery Bypass Grafting: A Single-Center Experience
- PMID: 38480660
- PMCID: PMC11052859
- DOI: 10.1007/s12325-024-02805-0
Perioperative and Long-Term Outcomes in Patients Undergoing Synchronous Carotid Endarterectomy and Coronary Artery Bypass Grafting: A Single-Center Experience
Abstract
Introduction: Patients requiring coronary artery bypass grafting (CABG) and carotid endarterectomy (CEA) can be managed with staged (CEA before CABG), reverse staged (CABG before CEA) or synchronous treatment. This single-center retrospective study evaluated the outcomes in patients undergoing planned synchronous CEA and CABG.
Methods: Between 2000 and 2020 a total of 185 patients with symptomatic triple-vessel or left main coronary artery disease associated with 70-99% asymptomatic or 50-99% symptomatic uni- or bilateral internal carotid artery (ICA) stenosis underwent synchronous CEA and CABG at our institution. Study endpoints were defined as mortality, stroke and myocardial infarction at 30 days. Additionally, the composite endpoint of these events was investigated.
Results: At 30 days, mortality, stroke and myocardial infarction rates were 5.9%, 8.1% (permanent [unresolved deficit at discharge] 5.4%) and 3.8%, respectively, and the composite endpoint was reached in 13.0% of patients. Patients suffering from a stroke more frequently had a contralateral 70-99% ICA stenosis (60.0% vs. 17.3%; p < 0.001), peripheral artery disease (73.3% vs. 38.9%; p = 0.013) and prolonged cardiopulmonary bypass time (mean 119 ± 62 min vs. 84 ± 29 min; p = 0.012). Multivariate logistic regression analysis revealed the duration of cardiopulmonary bypass (odds ratio [OR] 1.024; 95% confidence interval [CI] 1.002-1.046; p = 0.034), a history of type 2 diabetes mellitus (OR 5.097; 95% CI 1.161-22.367; p = 0.031) and peripheral artery disease (OR 5.814; 95% CI 1.231-27.457; p = 0.026) as independent risk factors for reaching the composite endpoint.
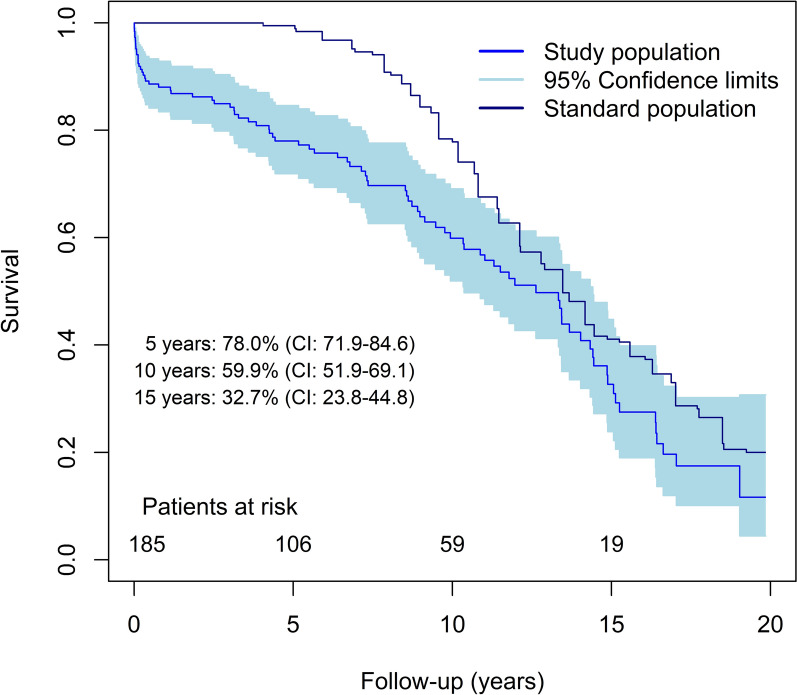
Conclusion: Patients undergoing synchronous CEA and CABG face an elevated risk of perioperative cardiovascular events, particularly an increased stroke risk in patients with symptomatic and bilateral ICA stenosis. Graphical Abstract available for this article.
Keywords: Carotid endarterectomy; Coronary artery bypass grafting; Internal carotid artery stenosis; Long-term survival; Perioperative stroke.
© 2024. The Author(s).
Conflict of interest statement
Paimann Nawrozi, Thomas Ratschiller, Wolfgang Schimetta, Gregor Gierlinger, Markus Pirklbauer, Hannes Müller and Andreas Zierer declare no conflicts of interest related to this study.
Figures

Similar articles
-
Outcomes of simultaneous carotid endarterectomy and coronary artery bypass grafting: A single centre experience.Vascular. 2023 Oct;31(5):914-921. doi: 10.1177/17085381221098281. Epub 2022 May 1. Vascular. 2023. PMID: 35491987
-
Assessment of atherosclerotic plaque morphology using contrast-enhanced ultrasound and its impact on primary cardiovascular events following simultaneous carotid endarterectomy and coronary artery bypass grafting.Vascular. 2025 Feb;33(1):205-211. doi: 10.1177/17085381241239499. Epub 2024 Mar 13. Vascular. 2025. PMID: 38479436
-
Operative and long-term outcomes of combined and staged carotid endarterectomy and coronary bypass.J Vasc Surg. 2023 May;77(5):1424-1433.e1. doi: 10.1016/j.jvs.2023.01.015. Epub 2023 Jan 18. J Vasc Surg. 2023. PMID: 36681256 Free PMC article.
-
Synchronous versus Staged Carotid Endarterectomy and Coronary Artery Bypass Graft for Patients with Concomitant Severe Coronary and Carotid Artery Stenosis: A Systematic Review and Meta-analysis.Ann Vasc Surg. 2020 Feb;63:427-438.e1. doi: 10.1016/j.avsg.2019.09.007. Epub 2019 Oct 17. Ann Vasc Surg. 2020. PMID: 31629126
-
Should patients with asymptomatic significant carotid stenosis undergo simultaneous carotid and cardiac surgery?Interact Cardiovasc Thorac Surg. 2014 Apr;18(4):511-8. doi: 10.1093/icvts/ivt525. Epub 2013 Dec 23. Interact Cardiovasc Thorac Surg. 2014. PMID: 24368551 Free PMC article. Review.
References
-
- Illuminati G, Ricco J-B, Caliò F, et al. Short-term results of a randomized trial examining timing of carotid endarterectomy in patients with severe asymptomatic unilateral carotid stenosis undergoing coronary artery bypass grafting. J Vasc Surg. 2011;54(4):993–999. doi: 10.1016/j.jvs.2011.03.284. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
