

Proteogenomic analysis of enriched HGSOC tumor epithelium identifies prognostic signatures and therapeutic vulnerabilities
- PMID: 38480868
- PMCID: PMC10937683
- DOI: 10.1038/s41698-024-00519-8
Proteogenomic analysis of enriched HGSOC tumor epithelium identifies prognostic signatures and therapeutic vulnerabilities
Erratum in
-
Author Correction: Proteogenomic analysis of enriched HGSOC tumor epithelium identifies prognostic signatures and therapeutic vulnerabilities.NPJ Precis Oncol. 2024 May 6;8(1):97. doi: 10.1038/s41698-024-00588-9. NPJ Precis Oncol. 2024. PMID: 38710993 Free PMC article. No abstract available.
Abstract
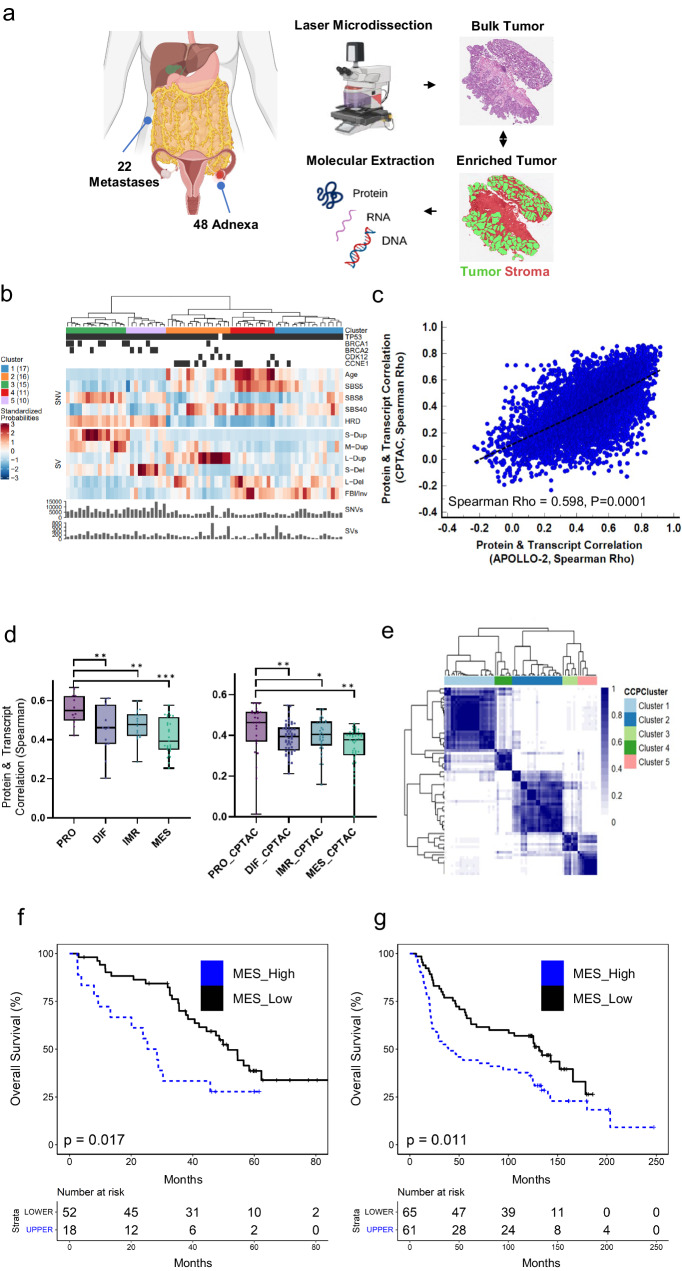
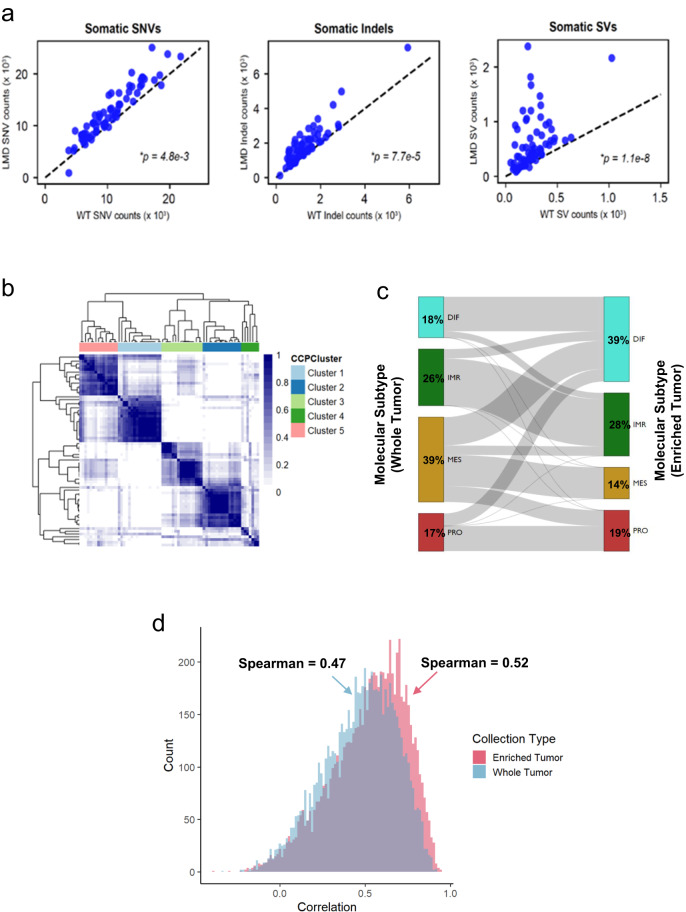
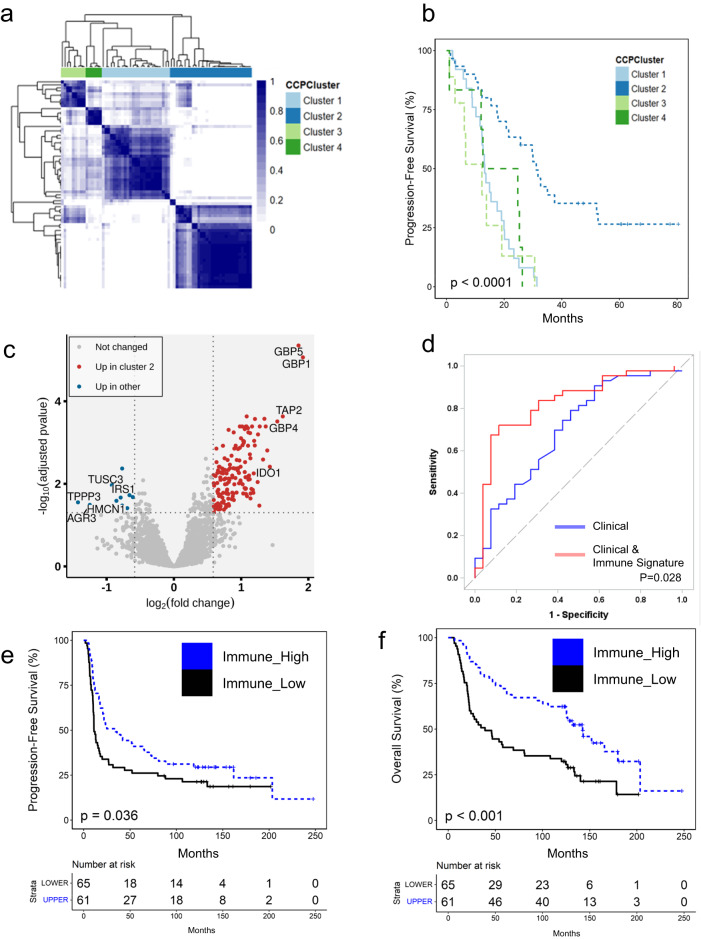
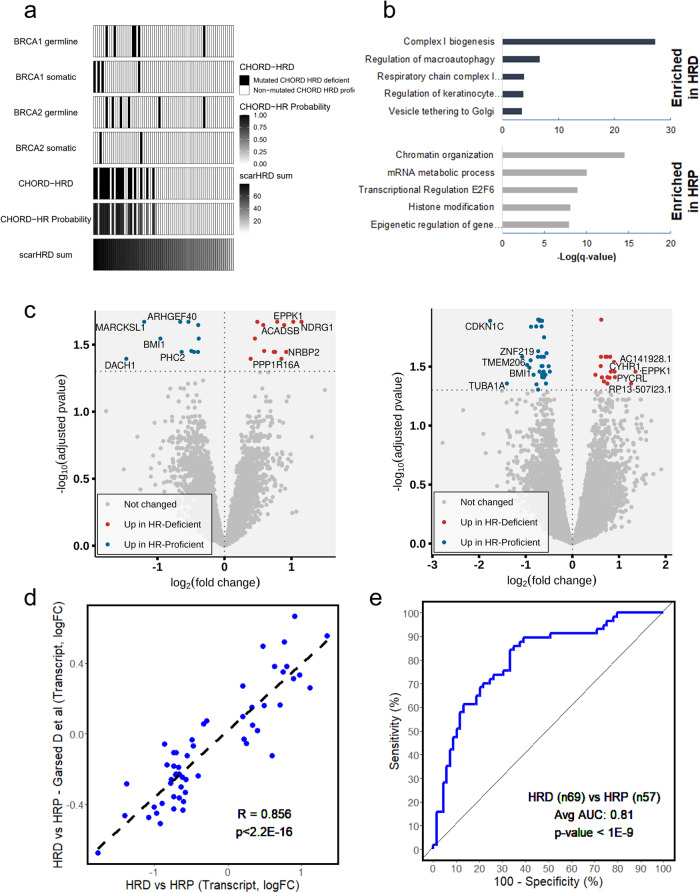
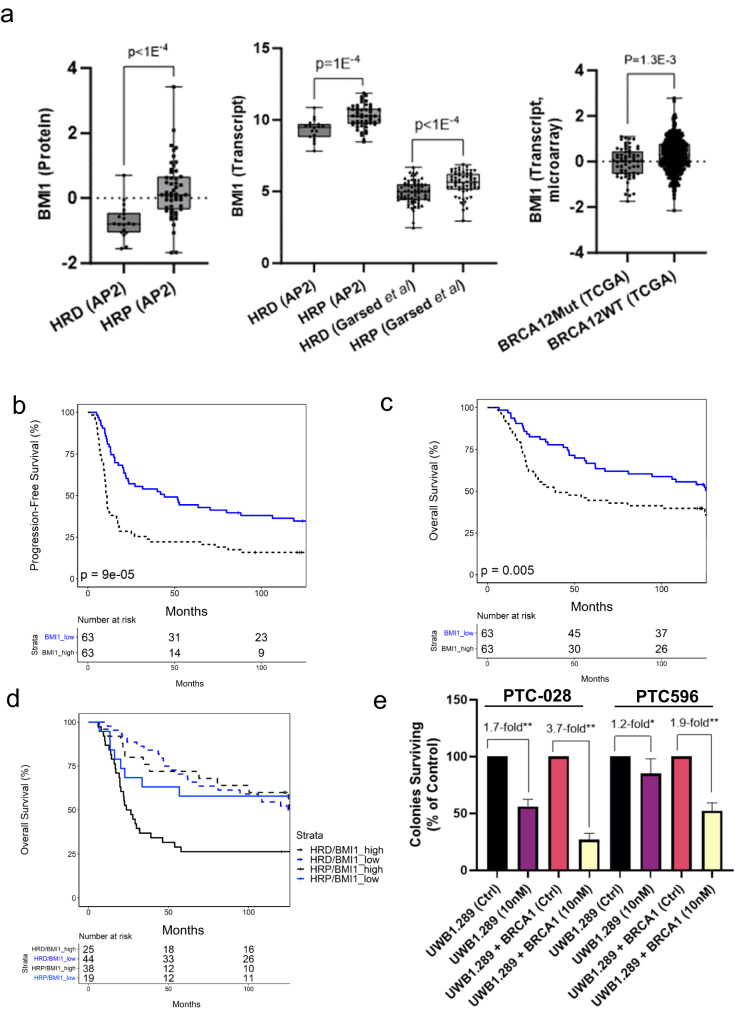
We performed a deep proteogenomic analysis of bulk tumor and laser microdissection enriched tumor cell populations from high-grade serous ovarian cancer (HGSOC) tissue specimens spanning a broad spectrum of purity. We identified patients with longer progression-free survival had increased immune-related signatures and validated proteins correlating with tumor-infiltrating lymphocytes in 65 tumors from an independent cohort of HGSOC patients, as well as with overall survival in an additional 126 HGSOC patient cohort. We identified that homologous recombination deficient (HRD) tumors are enriched in pathways associated with metabolism and oxidative phosphorylation that we validated in independent patient cohorts. We further identified that polycomb complex protein BMI-1 is elevated in HR proficient (HRP) tumors, that elevated BMI-1 correlates with poor overall survival in HRP but not HRD HGSOC patients, and that HRP HGSOC cells are uniquely sensitive to BMI-1 inhibition.
© 2024. The Author(s).
Conflict of interest statement
N.W.B., T.A., D.G., A.P., D.B., T.P.C., and G.L.M. are inventors for a provisional patent application related to findings reported in this manuscript. E.F.P. is a consultant for and shareholder of Perthera, Inc. and a consultant for Theralink Technologies, Inc. M.P. is a consultant for Theralink Technologies, Inc. D.D.L.B. receives grant funding from Genentech-Roche, Astra Zeneca, Beigene, and is a consultant to Exo Therapeutics. G.L.M. is a consultant for Kiyatec, GSK, and Merck. T.P.C. is a ThermoFisher Scientific, Inc SAB member and receives research funding from AbbVie.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
