

Circulating 25-hydroxyvitamin D and survival outcomes of colorectal cancer: evidence from population-based prospective cohorts and Mendelian randomisation
- PMID: 38480934
- PMCID: PMC11058806
- DOI: 10.1038/s41416-024-02643-5
Circulating 25-hydroxyvitamin D and survival outcomes of colorectal cancer: evidence from population-based prospective cohorts and Mendelian randomisation
Abstract
Background: To investigate the association between circulating 25-hydroxyvitamin D (25-OHD) and colorectal cancer (CRC) survival outcomes.
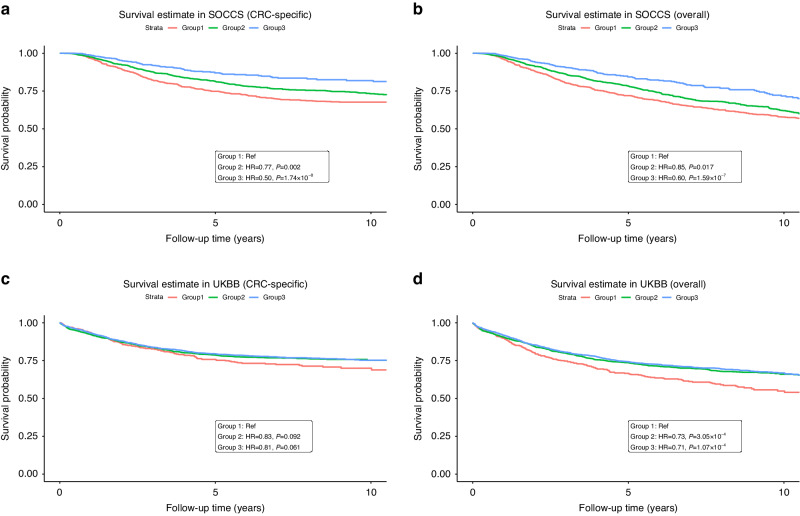
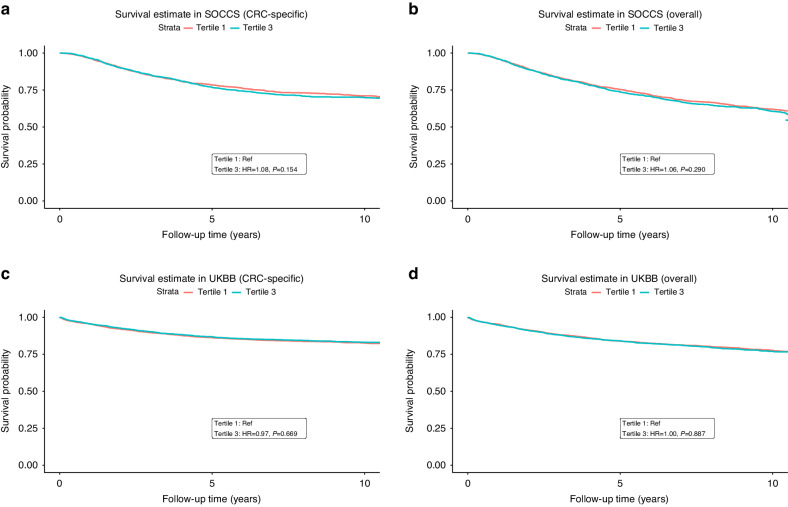
Methods: We conducted analyses among the Study of Colorectal Cancer in Scotland (SOCCS) and the UK Biobank (UKBB). Both cancer-specific survival (CSS) and overall survival (OS) outcomes were examined. The 25-OHD levels were categorised into three groups, and multi-variable Cox-proportional hazard models were applied to estimate hazard ratios (HRs). We performed individual-level Mendelian randomisation (MR) through the generated polygenic risk scores (PRS) of 25-OHD and summary-level MR using the inverse-variance weighted (IVW) method.
Results: We observed significantly poorer CSS (HR = 0.65,95%CI = 0.55-0.76,P = 1.03 × 10-7) and OS (HR = 0.66,95%CI = 0.58-0.75,P = 8.15 × 10-11) in patients with the lowest compared to those with the highest 25-OHD after adjusting for covariates. These associations remained across patients with varied tumour sites and stages. However, we found no significant association between 25-OHD PRS and either CSS (HR = 0.98,95%CI = 0.80-1.19,P = 0.83) or OS (HR = 1.07,95%CI = 0.91-1.25,P = 0.42). Furthermore, we found no evidence for causal effects by conducting summary-level MR analysis for either CSS (IVW:HR = 1.04,95%CI = 0.85-1.28,P = 0.70) or OS (IVW:HR = 1.10,95%CI = 0.93-1.31,P = 0.25).
Conclusion: This study supports the observed association between lower circulating 25-OHD and poorer survival outcomes for CRC patients. Whilst the genotype-specific association between better outcomes and higher 25-OHD is intriguing, we found no support for causality using MR approaches.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
