

Immune profiles of pre-frail people living with HIV-1: a prospective longitudinal study
- PMID: 38481213
- PMCID: PMC10935995
- DOI: 10.1186/s12979-024-00416-5
Immune profiles of pre-frail people living with HIV-1: a prospective longitudinal study
Abstract
Background: People living with HIV (PLWH) are at risk of frailty, which is predictive for death. As an overactivity of the immune system is thought to fuel frailty, we characterized the immune activation profiles linked to frailty.
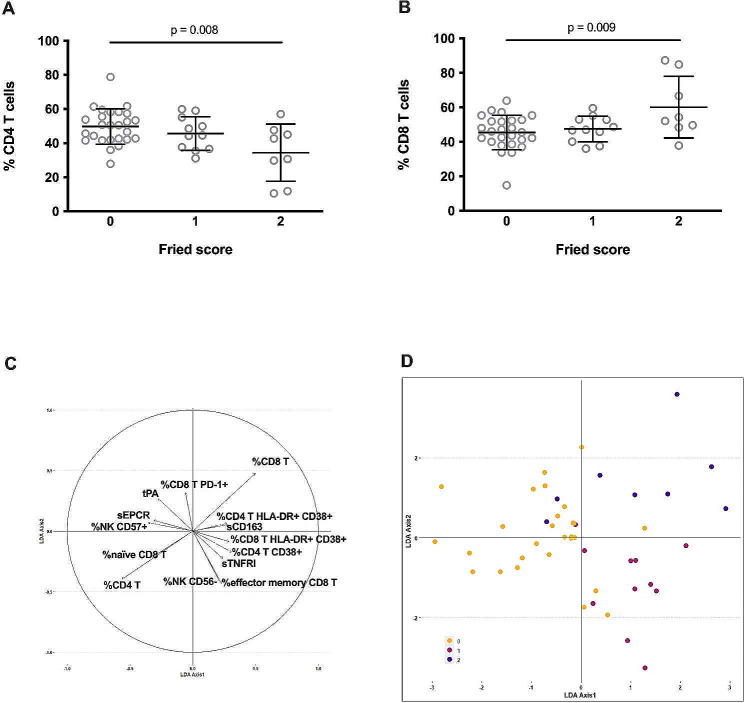
Methods: We quantified twenty-seven activation markers in forty-six virological responders (four females and forty-two males; median age, 74 years; median duration of infection, 24 years; median duration of undetectability, 13 years), whose frailty was determined according to the Fried criteria. T cell and NK cell activation was evaluated by flow cytometry, using a panel of cell surface markers. Soluble markers of inflammation, and monocyte activation and endothelial activation were measured by ELISA. The participants' immune activation was profiled by an unsupervised double hierarchical clustering analysis. We used ANOVA p-values to rank immunomarkers most related to Fried score. A Linear Discriminant Analysis (LDA) was performed to link immune activation markers to frailty.
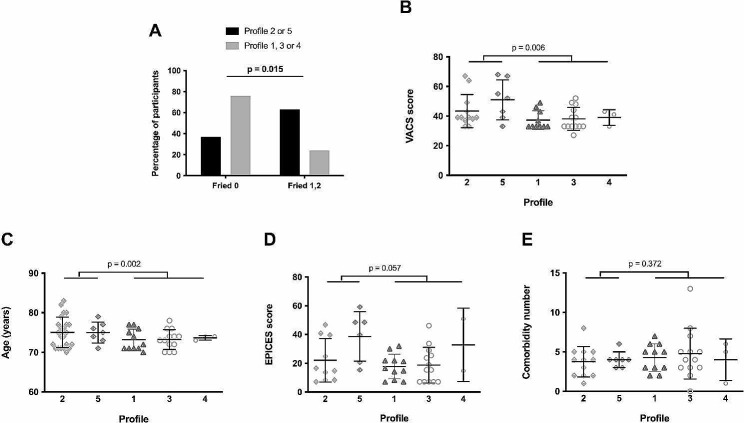
Results: 41% of the participants were pre-frail, including 24% with a Fried score of 1, and 17% with a Fried score of 2. ANOVA identified the 14 markers of T cell, monocyte, NK cell, endothelial activation, and inflammation the most linked to Fried 3 classes. The LDA performed with these 14 markers was capable of discriminating volunteers according to their Fried score. Two out of the 5 immune activation profiles revealed by the hierarchical clustering were linked to and predictive of pre-frailty. These two profiles were characterized by a low percentage of CD4 T cells and a high percentage of CD8 T cells, activated CD4 T cells, CD8 T cells, and NK cells, and inflammation.
Conclusions: We identified a particular immune activation profile associated with pre-frailty in PLWH. Profiling participants at risk of developing frailty might help to tailor the screening and prevention of medical complications fueled by loss of robustness. Further studies will indicate whether this frailty signature is specific or not of HIV infection, and whether it also precedes frailty in the general population.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
-
- Kooij KW, Wit FW, Schouten J, van der Valk M, Godfried MH, Stolte IG, et al. HIV infection is independently associated with frailty in middle-aged HIV type 1-infected individuals compared with similar but uninfected controls. AIDS. 2016;30(2):241–50. doi: 10.1097/QAD.0000000000000910. - DOI - PubMed
-
- Justice AC, Freiberg MS, Tracy R, Kuller L, Tate JP, Goetz MB, et al. Does an index composed of clinical data reflect effects of inflammation, coagulation, and monocyte activation on mortality among those aging with HIV? Clin Infect Dis. 2012;54(7):984–94. doi: 10.1093/cid/cir989. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
