

Fact vs. fiction: naloxone in the treatment of opioid-induced respiratory depression in the current era of synthetic opioids
- PMID: 38481848
- PMCID: PMC10933112
- DOI: 10.3389/fpubh.2024.1346109
Fact vs. fiction: naloxone in the treatment of opioid-induced respiratory depression in the current era of synthetic opioids
Abstract
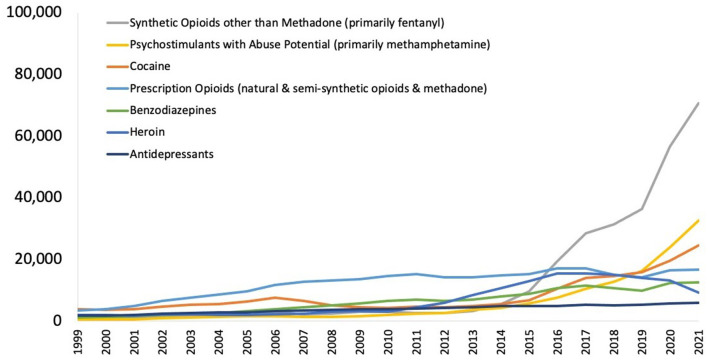
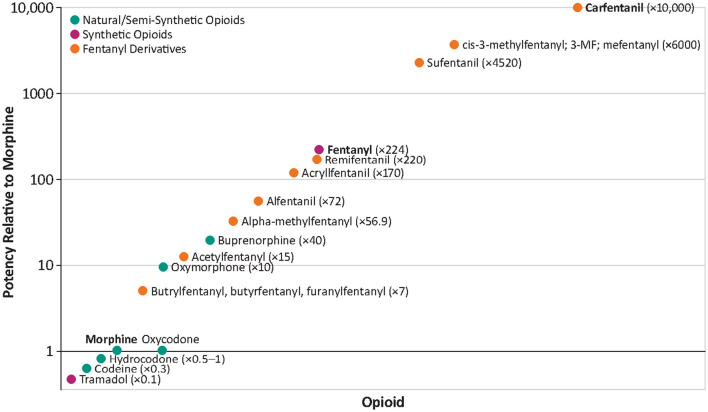
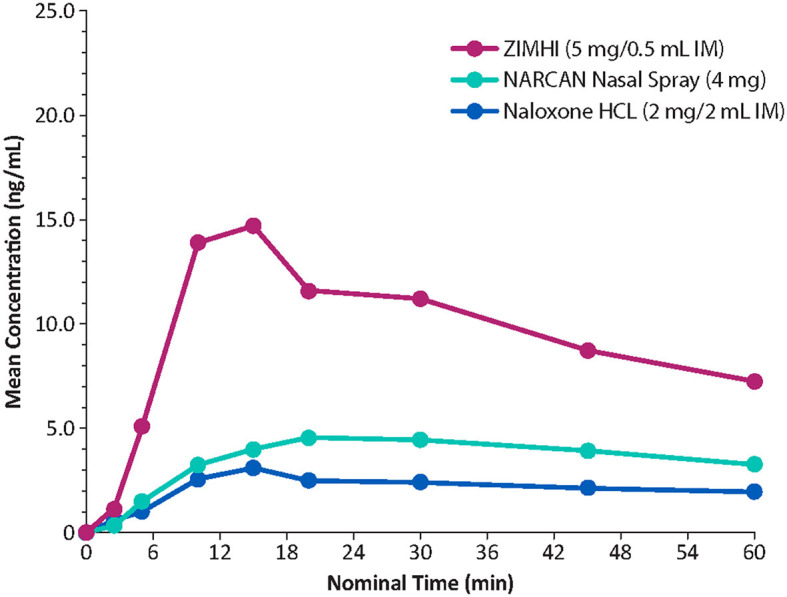
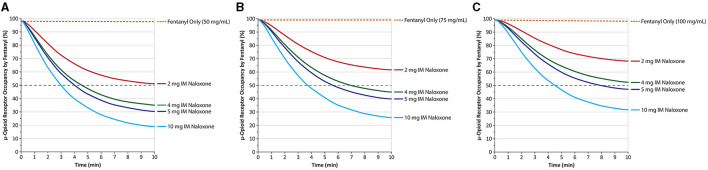
Opioid-induced respiratory depression (OIRD) deaths are ~80,000 a year in the US and are a major public health issue. Approximately 90% of fatal opioid-related deaths are due to synthetic opioids such as fentanyl, most of which is illicitly manufactured and distributed either on its own or as an adulterant to other drugs of abuse such as cocaine or methamphetamine. Other potent opioids such as nitazenes are also increasingly present in the illicit drug supply, and xylazine, a veterinary tranquilizer, is a prevalent additive to opioids and other drugs of abuse. Naloxone is the main treatment used to reverse OIRD and is available as nasal sprays, prefilled naloxone injection devices, and generic naloxone for injection. An overdose needs to be treated as soon as possible to avoid death, and synthetic opioids such as fentanyl are up to 50 times more potent than heroin, so the availability of new, higher-dose, 5-mg prefilled injection or 8-mg intranasal spray naloxone preparations are important additions for emergency treatment of OIRDs, especially by lay people in the community. Higher naloxone doses are expected to reverse a synthetic overdose more rapidly and the current formulations are ideal for use by untrained lay people in the community. There are potential concerns about severe withdrawal symptoms, or pulmonary edema from treatment with high-dose naloxone. However, from the perspective of first responders, the balance of risks would point to administration of naloxone at the dose required to combat the overdose where the risk of death is very high. The presence of xylazines as an adulterant complicates the treatment of OIRDs, as naloxone is probably ineffective, although it will reverse the respiratory depression due to the opioid. For these patients, hospitalization is particularly vital. Education about the benefits of naloxone remains important not only in informing people about how to treat emergency OIRDs but also how to obtain naloxone. A call to emergency services is also essential after administering naloxone because, although the patient may revive, they may overdose again later because of the short half-life of naloxone and the long-lasting potency of fentanyl and its analogs.
Keywords: drug abuse; fentanyl; naloxone; nitazene; opioid; opioid-induced respiratory depression; xylazine.
Copyright © 2024 Dahan, Franko, Carroll, Craig, Crow, Galinkin, Garrity, Peterson and Rausch.
Conflict of interest statement
AD received consultancy fees from Enalare Therapeutics Inc. (Princeton, New Jersey), Trevena Inc. (Chesterbroom, New Jersey), and awards or grants from the U.S. Food and Drug Administration (Silver Spring, Maryland), the Netherlands Organization for Health Research and Development, and the Dutch Research Council (the Hague, the Netherlands). TF is a consultant for Wolters-Kluwer. DC has received consulting fees, within the past 12 months, from AbbVie, Inc. (Chicago, IL), Collegium Pharmaceutical, Inc. (Stoughton, MA), Purdue Pharma (Stamford, CT), and Endo Pharmaceuticals (Malvern, PA). JP is the Founder and Executive Director of Learn to Cope, Inc., a registered 501(c)3 non-profit organization providing 100% free resources and support to families dealing with addiction and recovery. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
References
-
- National Center for Health Statistics . Provisional Data Shows U.S. Drug Overdose Deaths Top 100,000 in 2022 (2023). Available online at: https://blogs.cdc.gov/nchs/2023/05/18/7365/# (accessed February 12, 2024).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous