

Efficacy and safety of bispecific antibodies therapy for relapsed or refractory multiple myeloma: a systematic review and meta-analysis of prospective clinical trials
- PMID: 38482019
- PMCID: PMC10933024
- DOI: 10.3389/fimmu.2024.1348955
Efficacy and safety of bispecific antibodies therapy for relapsed or refractory multiple myeloma: a systematic review and meta-analysis of prospective clinical trials
Abstract
Objective: Bispecific antibody (BsAbs) therapy represents a promising immunotherapeutic approach with manageable toxicity and noteworthy preliminary efficacy in treating patients with relapsed or refractory multiple myeloma (RRMM). The objective of this systematic review and meta-analysis was to compare the efficacy and safety of B-cell maturation antigen (BCMA)-targeted BsAbs and non-BCMA-targeted BsAbs in the treatment of RRMM patients.
Methods: PubMed/MEDLINE, Web of Science, EMBASE, Cochrane Library and meeting libraries were searched from inception to August 16th, 2023. The efficacy evaluation included the complete objective response rate (ORR), complete response (CR) rate, stringent CR (sCR) rate, partial response (PR) rate, and very good PR (VGPR) rate. The efficacy evaluation included any grade adverse events (AEs) and grade ≥ 3 AEs.
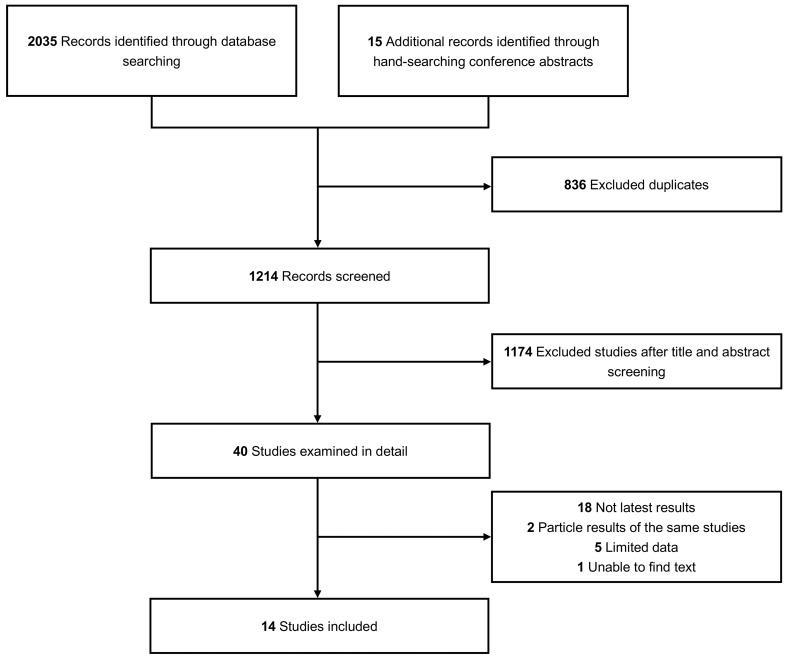
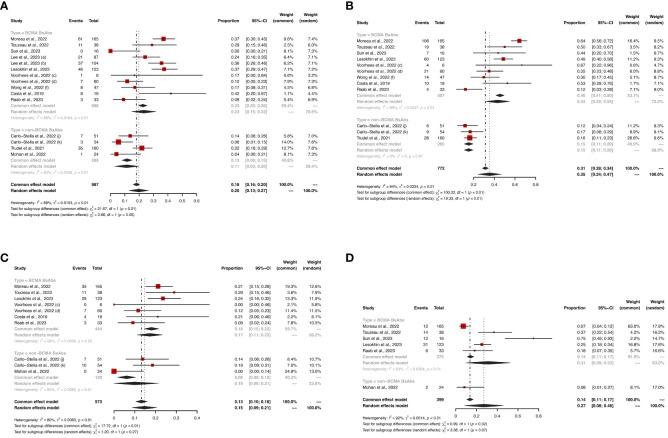
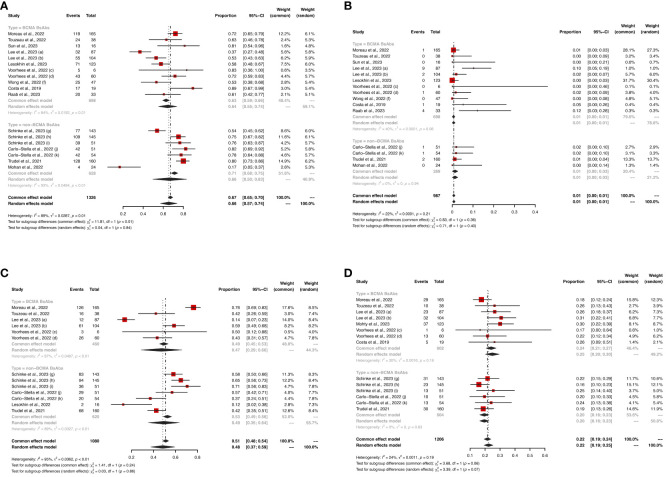
Results: Fourteen studies with a total of 1473 RRMM patients were included. The pooled ORR of the entire cohort was 61%. The non-BCMA-targeted BsAbs group displayed a higher ORR than the BCMA-targeted BsAbs group (74% vs. 54%, P < 0.01). In terms of hematological AEs, BCMA-targeted BsAbs therapy exhibited higher risks of neutropenia (any grade: 48% vs. 18%, P < 0.01; grade ≥ 3: 43% vs. 15%, P < 0.01) and lymphopenia (any grade: 37% vs. 8%, P < 0.01; grade ≥ 3: 31% vs. 8%, P = 0.07). Regarding non-hematological AEs, there were no significant differences in the risks of cytokine release syndrome (CRS, any grade: 64% vs. 66%, P = 0.84; grade ≥ 3: 1% vs. 1%, P = 0.36) and infections (any grade: 47% vs. 49%, P = 0.86; grade ≥ 3: 24% vs. 20%, P = 0.06) between the two groups. However, non-BCMA-targeted BsAbs therapy was associated with a higher risk of immune effector cell-associated neurotoxicity syndrome (ICANS, any grade: 11% vs. 2%, P < 0.01) and lower risks of fatigue (any grade: 14% vs. 30%, P < 0.01) and pyrexia (any grade: 14% vs. 29%, P < 0.01).
Conclusion: This analysis suggest that non-BCMA-targeted BsAbs therapy may offer a more favorable treatment response and tolerability, while BCMA-targeted BsAbs therapy may be associated with diminished neurotoxic effects.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/, identifier CRD42018090768.
Keywords: bispecific antibodies; efficacy; immunotherapy; multiple myeloma; safety.
Copyright © 2024 Wang, Zhao, Zhu and Niu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
Effectiveness and safety of teclistamab for relapsed or refractory multiple myeloma: a systematic review and meta-analysis.Front Immunol. 2025 Apr 25;16:1565407. doi: 10.3389/fimmu.2025.1565407. eCollection 2025. Front Immunol. 2025. PMID: 40352937 Free PMC article.
-
Efficacy and Safety of CAR-Modified T Cell Therapy in Patients with Relapsed or Refractory Multiple Myeloma: A Meta-Analysis of Prospective Clinical Trials.Front Pharmacol. 2020 Dec 3;11:544754. doi: 10.3389/fphar.2020.544754. eCollection 2020. Front Pharmacol. 2020. PMID: 33343342 Free PMC article. Review.
-
Comprehensive assessment of adverse event profiles associated with bispecific antibodies in multiple myeloma.Blood Cancer J. 2025 Aug 1;15(1):130. doi: 10.1038/s41408-025-01334-5. Blood Cancer J. 2025. PMID: 40750760 Free PMC article.
-
The Role of Bispecific Antibodies in Relapsed Refractory Multiple Myeloma: A Systematic Review.Antibodies (Basel). 2023 May 29;12(2):38. doi: 10.3390/antib12020038. Antibodies (Basel). 2023. PMID: 37366654 Free PMC article. Review.
-
Safety and efficacy of T-cell-redirecting bispecific antibodies for patients with multiple myeloma: a systematic review and meta-analysis.Cancer Cell Int. 2023 Sep 5;23(1):193. doi: 10.1186/s12935-023-03045-y. Cancer Cell Int. 2023. PMID: 37670301 Free PMC article. Review.
Cited by
-
The silent signals: emerging safety concerns in bispecific antibody therapy for multiple myeloma.Front Med (Lausanne). 2025 Aug 13;12:1593405. doi: 10.3389/fmed.2025.1593405. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40880759 Free PMC article.
-
Bispecific antibodies combined with chemotherapy in solid tumor treatment, the path forward?Front Immunol. 2025 Apr 25;16:1568724. doi: 10.3389/fimmu.2025.1568724. eCollection 2025. Front Immunol. 2025. PMID: 40352940 Free PMC article.
-
Navigating the Economic Burden of Multiple Myeloma: Insights into Cost-effectiveness of CAR-T and Bispecific Antibody Therapies.Curr Hematol Malig Rep. 2025 Jan 4;20(1):3. doi: 10.1007/s11899-024-00748-5. Curr Hematol Malig Rep. 2025. PMID: 39754658 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials