

Feasibility of a Self-directed Upper Extremity Training Program to Promote Actual Arm Use for Individuals Living in the Community With Chronic Stroke
- PMID: 38482107
- PMCID: PMC10928291
- DOI: 10.1016/j.arrct.2023.100316
Feasibility of a Self-directed Upper Extremity Training Program to Promote Actual Arm Use for Individuals Living in the Community With Chronic Stroke
Abstract
Objective: To determine the feasibility of a self-directed training protocol to promote actual arm use in everyday life. The secondary aim was to explore the initial efficacy on upper extremity (UE) outcome measures.
Design: Feasibility study using multiple methods.
Setting: Home and outpatient research lab.
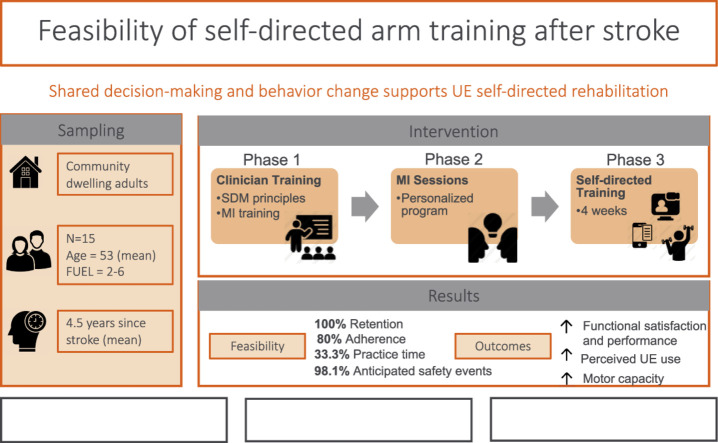
Participants: Fifteen adults (6 women, 9 men, mean age=53.08 years) with chronic stroke living in the community. There was wide range of UE functional levels, ranging from dependent stabilizer (limited function) to functional assist (high function).
Intervention: Use My Arm-Remote protocol. Phase 1 consisted of clinician training on motivational interviewing (MI). Phase 2 consisted of MI sessions with participants to determine participant generated goals, training activities, and training schedules. Phase 3 consisted of UE task-oriented training (60 minutes/day, 5 days/week, for 4 weeks). Participants received daily surveys through an app to monitor arm training behavior and weekly virtual check-ins with clinicians to problem-solve challenges and adjust treatment plans.
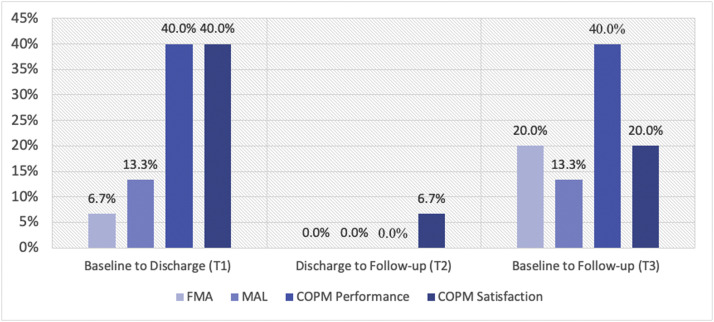
Outcome measures: Primary outcome measures were feasibility domains after intervention, measured by quantitative study data and qualitative semi-structured interviews. Secondary outcomes included the Canadian Occupational Performance Measure (COPM), Motor Activity Log (MAL), Fugl-Meyer Assessment (FMA), and accelerometry-based duration of use metric measured at baseline, discharge, and 4-week follow-up.
Results: The UMA-R was feasible in the following domains: recruitment rate, retention rate, intervention acceptance, intervention delivery, adherence frequency, and safety. Adherence to duration of daily practice did not meet our criteria. Improvements in UE outcomes were achieved at discharge and maintained at follow-up as measured by COPM-Performance subscale (F[1.42, 19.83]=17.72, P<.001) and COPM-Satisfaction subscale (F[2, 28]=14.73, P<.001), MAL (F[1.31, 18.30]=12.05, P<.01) and the FMA (F[2, 28]=16.62, P<.001).
Conclusion: The UMA-R was feasible and safe to implement for individuals living in the community with chronic stroke. Adherence duration was identified as area of refinement. Participants demonstrated improvements in standardized UE outcomes to support initial efficacy of the UMA-R. Shared decision-making and behavior change frameworks can support the implementation of UE self-directed rehabilitation. Our results warrant the refinement and further testing of the UMA-R.
Keywords: Actual arm use; Self-directed training; Shared decision-making; Stroke; Upper extremity.
© 2024 The Authors.
Figures

Similar articles
-
Protocol for a remote home-based upper extremity self-training program for community-dwelling individuals after stroke.Contemp Clin Trials Commun. 2023 Mar 17;33:101112. doi: 10.1016/j.conctc.2023.101112. eCollection 2023 Jun. Contemp Clin Trials Commun. 2023. PMID: 37113325 Free PMC article.
-
Optimization of Upper Extremity Rehabilitation by Combining Telerehabilitation With an Exergame in People With Chronic Stroke: Protocol for a Mixed Methods Study.JMIR Res Protoc. 2020 May 21;9(5):e14629. doi: 10.2196/14629. JMIR Res Protoc. 2020. PMID: 32097119 Free PMC article.
-
Therapeutic Instrumental Music Training and Motor Imagery in Post-Stroke Upper-Extremity Rehabilitation: A Randomized-Controlled Pilot Study.Arch Rehabil Res Clin Transl. 2021 Oct 8;3(4):100162. doi: 10.1016/j.arrct.2021.100162. eCollection 2021 Dec. Arch Rehabil Res Clin Transl. 2021. PMID: 34977544 Free PMC article.
-
Does noninvasive brain stimulation combined with other therapies improve upper extremity motor impairment, functional performance, and participation in activities of daily living after stroke? A systematic review and meta-analysis of randomized controlled trial.Top Stroke Rehabil. 2023 Apr;30(3):213-234. doi: 10.1080/10749357.2022.2026278. Epub 2022 Feb 3. Top Stroke Rehabil. 2023. PMID: 35112659
-
The Effect of Priming on Outcomes of Task-Oriented Training for the Upper Extremity in Chronic Stroke: A Systematic Review and Meta-analysis.Neurorehabil Neural Repair. 2020 Jun;34(6):479-504. doi: 10.1177/1545968320912760. Epub 2020 May 26. Neurorehabil Neural Repair. 2020. PMID: 32452242
Cited by
-
Clinician and patient experiences with shared decision-making to promote daily arm use for individuals with chronic stroke: an exploratory qualitative study.Front Rehabil Sci. 2024 Sep 19;5:1414878. doi: 10.3389/fresc.2024.1414878. eCollection 2024. Front Rehabil Sci. 2024. PMID: 39363988 Free PMC article.
-
High-Dose, High-Intensity Stroke Rehabilitation: Why Aren't We Giving It?Stroke. 2025 May;56(5):1351-1364. doi: 10.1161/STROKEAHA.124.043650. Epub 2025 Apr 28. Stroke. 2025. PMID: 40294175
References
-
- Kochanek KD, Murphy SL, Xu J, Arias E. Mortality in the United States, 2013. NCHS Data Brief. 2014;(178):1–8. - PubMed
-
- Benjamin EJ, Virani SS, Callaway CW, et al. Heart Disease and Stroke Statistics-2018 Update: a report From the American Heart Association. Circulation. 2018;137:e67–492. - PubMed
-
- Broeks JG, Lankhorst GJ, Rumping K, Prevo AJ. The long-term outcome of arm function after stroke: results of a follow-up study. Disabil Rehabil. 1999;21:357–364. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
