

In vitro activity of cefiderocol against European Pseudomonas aeruginosa and Acinetobacter spp., including isolates resistant to meropenem and recent β-lactam/β-lactamase inhibitor combinations
- PMID: 38483164
- PMCID: PMC10986614
- DOI: 10.1128/spectrum.03836-23
In vitro activity of cefiderocol against European Pseudomonas aeruginosa and Acinetobacter spp., including isolates resistant to meropenem and recent β-lactam/β-lactamase inhibitor combinations
Abstract
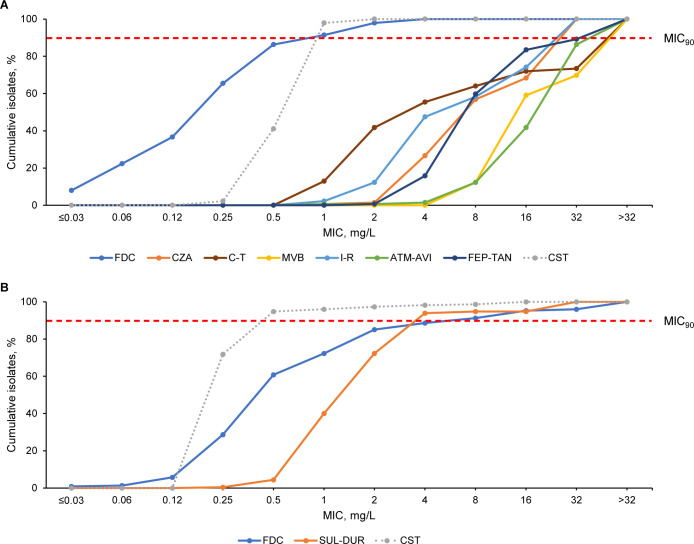
Carbapenem-resistant Pseudomonas aeruginosa and Acinetobacter spp. represent major threats and have few approved therapeutic options. Non-fermenting Gram-negative isolates were collected from hospitalized inpatients from 49 sites in 6 European countries between 01 January 2020 and 31 December 2020 and underwent susceptibility testing against cefiderocol and β-lactam/β-lactamase inhibitor combinations. Meropenem-resistant (MIC >8 mg/L), cefiderocol-susceptible isolates were analyzed by PCR, and cefiderocol-resistant isolates were analyzed by whole-genome sequencing to identify resistance mechanisms. Overall, 1,451 (950 P. aeruginosa; 501 Acinetobacter spp.) isolates were collected, commonly from the respiratory tract (42.0% and 39.3%, respectively). Cefiderocol susceptibility was higher than β-lactam/β-lactamase inhibitor combinations against P. aeruginosa (98.9% vs 83.3%-91.4%), and P. aeruginosa resistant to meropenem (n = 139; 97.8% vs 12.2%-59.7%), β-lactam/β-lactamase inhibitor combinations (93.6%-98.1% vs 10.7%-71.8%), and both meropenem and ceftazidime-avibactam (96.7% vs 5.0%-45.0%) or ceftolozane-tazobactam (98.4% vs 8.1%-54.8%), respectively. Cefiderocol and sulbactam-durlobactam susceptibilities were high against Acinetobacter spp. (92.4% and 97.0%) and meropenem-resistant Acinetobacter spp. (n = 227; 85.0% and 93.8%) but lower against sulbactam-durlobactam- (n = 15; 13.3%) and cefiderocol- (n = 38; 65.8%) resistant isolates, respectively. Among meropenem-resistant P. aeruginosa and Acinetobacter spp., the most common β-lactamase genes were metallo-β-lactamases [30/139; blaVIM-2 (15/139)] and oxacillinases [215/227; blaOXA-23 (194/227)], respectively. Acquired β-lactamase genes were identified in 1/10 and 32/38 of cefiderocol-resistant P. aeruginosa and Acinetobacter spp., and pirA-like or piuA mutations in 10/10 and 37/38, respectively. Conclusion: cefiderocol susceptibility was high against P. aeruginosa and Acinetobacter spp., including meropenem-resistant isolates and those resistant to recent β-lactam/β-lactamase inhibitor combinations common in first-line treatment of European non-fermenters.
Importance: This was the first study in which the in vitro activity of cefiderocol and non-licensed β-lactam/β-lactamase inhibitor combinations were directly compared against Pseudomonas aeruginosa and Acinetobacter spp., including meropenem- and β-lactam/β-lactamase inhibitor combination-resistant isolates. A notably large number of European isolates were collected. Meropenem resistance was defined according to the MIC breakpoint for high-dose meropenem, ensuring that data reflect antibiotic activity against isolates that would remain meropenem resistant in the clinic. Cefiderocol susceptibility was high against non-fermenters, and there was no apparent cross resistance between cefiderocol and β-lactam/β-lactamase inhibitor combinations, with the exception of sulbactam-durlobactam. These results provide insights into therapeutic options for infections due to resistant P. aeruginosa and Acinetobacter spp. and indicate how early susceptibility testing of cefiderocol in parallel with β-lactam/β-lactamase inhibitor combinations will allow clinicians to choose the effective treatment(s) from all available options. This is particularly important as current treatment options against non-fermenters are limited.
Keywords: Acinetobacter spp.; Europe; Pseudomonas aeruginosa; aztreonam-avibactam; cefepime-taniborbactam; cefiderocol; ceftazidime-avibactam; ceftolozane-tazobactam; imipenem-relebactam; in vitro; meropenem; meropenem-resistant; meropenem-vaborbactam; resistance; sulbactam-durlobactam; β-lactamases; β-lactam/β-lactamase inhibitor combinations.
Conflict of interest statement
A.S.H. is an employee of Maxel Consulting ApS, Jyllinge, Denmark and is a contract employee of Shionogi B.V. Both K.J. and A.O. declare honoraria and grants from Shionogi, Pfizer, and MSD. I.M. is an employee of Antimicrobial Focus Ltd and was involved with the reporting of the study data by IHMA. C.L. is an employee of Shionogi B.V. J.D.P., M.W.P., and S.S. have no relevant conflicts of interest to disclose.
Figures
References
-
- European Centre for Disease Prevention and Control . 2022. Antimicrobial resistance in the EU/EEA (EARS-Net) - annual epidemiological report for 2021. Stockholm: ECDC
-
- World Health Organization . 2017. Prioritization of pathogens to guide discovery, research and development of new antibiotics for drug-resistant bacterial infections, including tuberculosis.
-
- Longshaw C, Manissero D, Tsuji M, Echols R, Yamano Y. 2020. In vitro activity of the siderophore cephalosporin, cefiderocol, against molecularly characterized, carbapenem-non-susceptible Gram-negative bacteria from Europe. JAC Antimicrob Resist 2:dlaa060. doi:10.1093/jacamr/dlaa060 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
