

Targeted therapies prime oncogene-driven lung cancers for macrophage-mediated destruction
- PMID: 38483480
- PMCID: PMC11060739
- DOI: 10.1172/JCI169315
Targeted therapies prime oncogene-driven lung cancers for macrophage-mediated destruction
Abstract
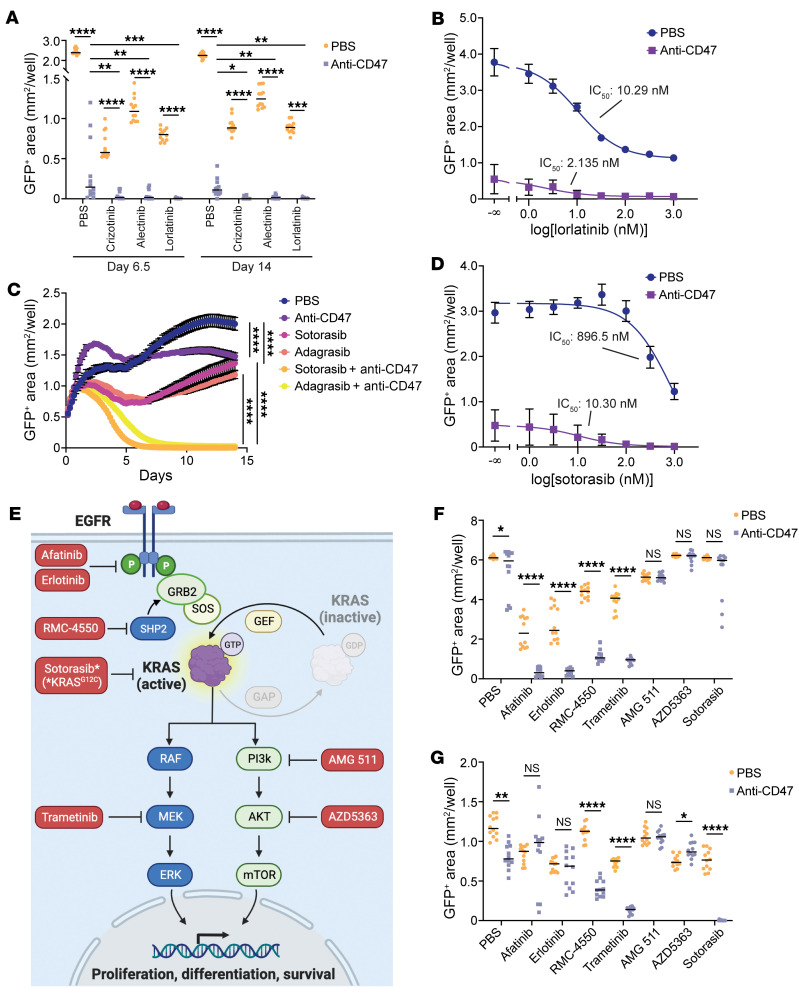
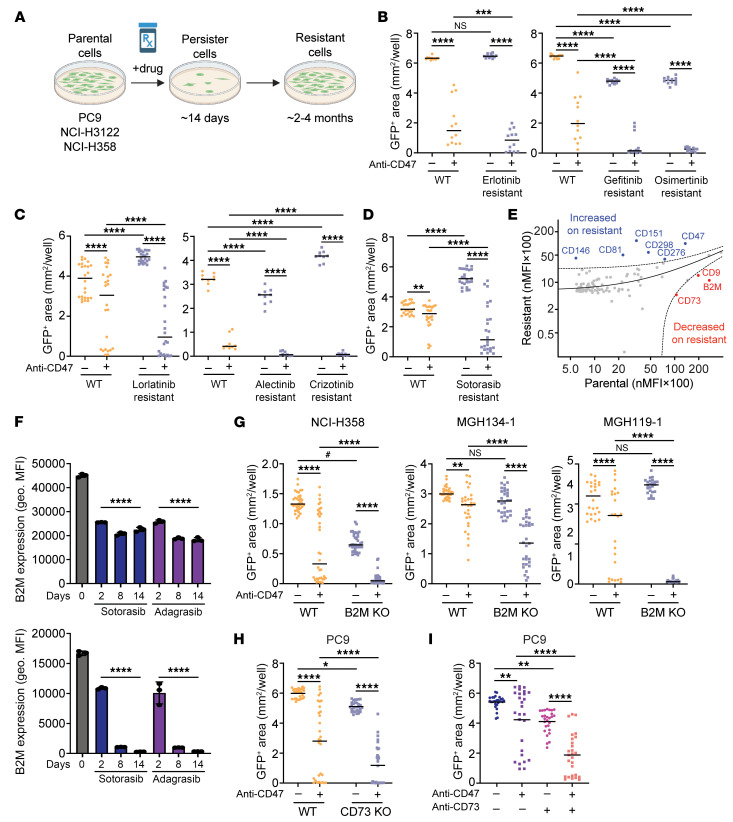
Macrophage immune checkpoint inhibitors, such as anti-CD47 antibodies, show promise in clinical trials for solid and hematologic malignancies. However, the best strategies to use these therapies remain unknown, and ongoing studies suggest they may be most effective when used in combination with other anticancer agents. Here, we developed an unbiased, high-throughput screening platform to identify drugs that render lung cancer cells more vulnerable to macrophage attack, and we found that therapeutic synergy exists between genotype-directed therapies and anti-CD47 antibodies. In validation studies, we found that the combination of genotype-directed therapies and CD47 blockade elicited robust phagocytosis and eliminated persister cells in vitro and maximized antitumor responses in vivo. Importantly, these findings broadly applied to lung cancers with various RTK/MAPK pathway alterations - including EGFR mutations, ALK fusions, or KRASG12C mutations. We observed downregulation of β2-microglobulin and CD73 as molecular mechanisms contributing to enhanced sensitivity to macrophage attack. Our findings demonstrate that dual inhibition of the RTK/MAPK pathway and the CD47/SIRPa axis is a promising immunotherapeutic strategy. Our study provides strong rationale for testing this therapeutic combination in patients with lung cancers bearing driver mutations.
Keywords: Cancer immunotherapy; Lung cancer; Macrophages; Oncology; Therapeutics.
Figures




Update of
-
Targeted therapies prime oncogene-driven lung cancers for macrophage-mediated destruction.bioRxiv [Preprint]. 2023 Mar 6:2023.03.03.531059. doi: 10.1101/2023.03.03.531059. bioRxiv. 2023. Update in: J Clin Invest. 2024 Mar 14;134(9):e169315. doi: 10.1172/JCI169315. PMID: 36945559 Free PMC article. Updated. Preprint.
References
-
- Jordan EJ, et al. Prospective comprehensive molecular characterization of lung adenocarcinomas for efficient patient matching to approved and emerging therapies. Cancer Discov. 2017;7(6):596–609. doi: 10.1158/2159-8290.CD-16-1337. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
