

Prognostic and Predictive Value of Immunoscore in Stage III Colorectal Cancer: Pooled Analysis of Cases From the SCOT and IDEA-HORG Studies
- PMID: 38484206
- PMCID: PMC11185918
- DOI: 10.1200/JCO.23.01648
Prognostic and Predictive Value of Immunoscore in Stage III Colorectal Cancer: Pooled Analysis of Cases From the SCOT and IDEA-HORG Studies
Abstract
Purpose: Immunoscore (IS) is prognostic in stage III colorectal cancer (CRC) and may predict benefit of duration (6 v 3 months) of adjuvant infusional fluorouracil, leucovorin, and oxaliplatin (FOLFOX) chemotherapy. We sought to determine IS prognostic and predictive value in stage-III CRC treated with adjuvant FOLFOX or oral capecitabine and infusional oxaliplatin (CAPOX) in the SCOT and IDEA-HORG trials.
Methods: Three thousand sixty-one cases had tumor samples, of which 2,643 (1,792 CAPOX) were eligible for IS testing. Predefined cutoffs (IS-Low and IS-High) were used to classify cases into two groups for analysis of disease-free survival (3-year DFS) and multivariable-adjusted hazard ratios (mvHRs) by Cox regression.
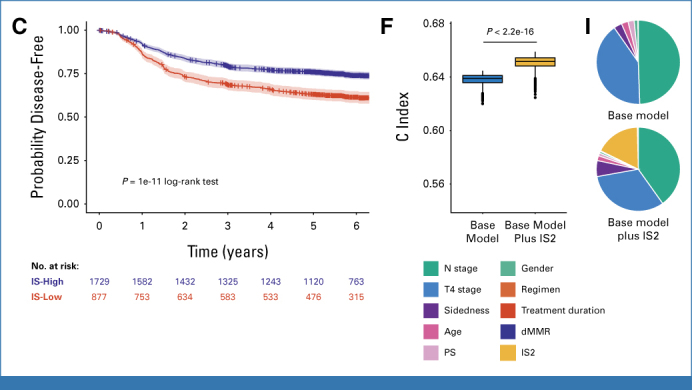
Results: IS was determined in 2,608 (99.5%) eligible cases, with 877 (33.7%) samples classified as IS-Low. IS-Low tumors were more commonly high-risk (T4 and/or N2; 52.9% IS-Low v 42.2% IS-High; P < .001) and in younger patients (P = .024). Patients with IS-Low tumors had significantly shorter DFS in the CAPOX, FOLFOX, and combined cohorts (mvHR, 1.52 [95% CI, 1.28 to 1.82]; mvHR, 1.58 [95% CI, 1.22 to 2.04]; and mvHR, 1.55 [95% CI, 1.34 to 1.79], respectively; P < .001 all comparisons), regardless of sex, BMI, clinical risk group, tumor location, treatment duration, or chemotherapy regimen. IS prognostic value was greater in younger (≤65 years) than older (>65 years) patients in the CAPOX cohort (mvHR, 1.92 [95% CI, 1.50 to 2.46] v 1.28 [95% CI, 1.01 to 1.63], PINTERACTION = .026), and in DNA mismatch repair proficient than deficient mismatch repair disease (mvHR, 1.68 [95% CI, 1.41 to 2.00] v 0.67 [95% CI, 0.30 to 1.49], PINTERACTION = .03), although these exploratory analyses were uncorrected for multiple testing. Adding IS to a model containing all clinical variables significantly improved prediction of DFS (likelihood ratio test, P < .001) regardless of MMR status.
Conclusion: IS is prognostic in stage III CRC treated with FOLFOX or CAPOX, including within clinically relevant tumor subgroups. Possible variation in IS prognostic value by age and MMR status, and prediction of benefit from extended adjuvant therapy merit validation.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures





References
-
- Sung H, Ferlay J, Siegel RL, et al. : Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71:209-249, 2021 - PubMed
-
- Cardoso R, Guo F, Heisser T, et al. : Colorectal cancer incidence, mortality, and stage distribution in European countries in the colorectal cancer screening era: An international population-based study. Lancet Oncol 22:1002-1013, 2021 - PubMed
-
- Argilés G, Tabernero J, Labianca R, et al. : Localised colon cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 31:1291-1305, 2020 - PubMed
-
- Andre T, Boni C, Mounedji-Boudiaf L, et al. : Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med 350:2343-2351, 2004 - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
