

Hormonal Contraception and Risk of Cardiometabolic Disease in Women with HIV
- PMID: 38484324
- PMCID: PMC11302212
- DOI: 10.1089/jwh.2023.0230
Hormonal Contraception and Risk of Cardiometabolic Disease in Women with HIV
Abstract
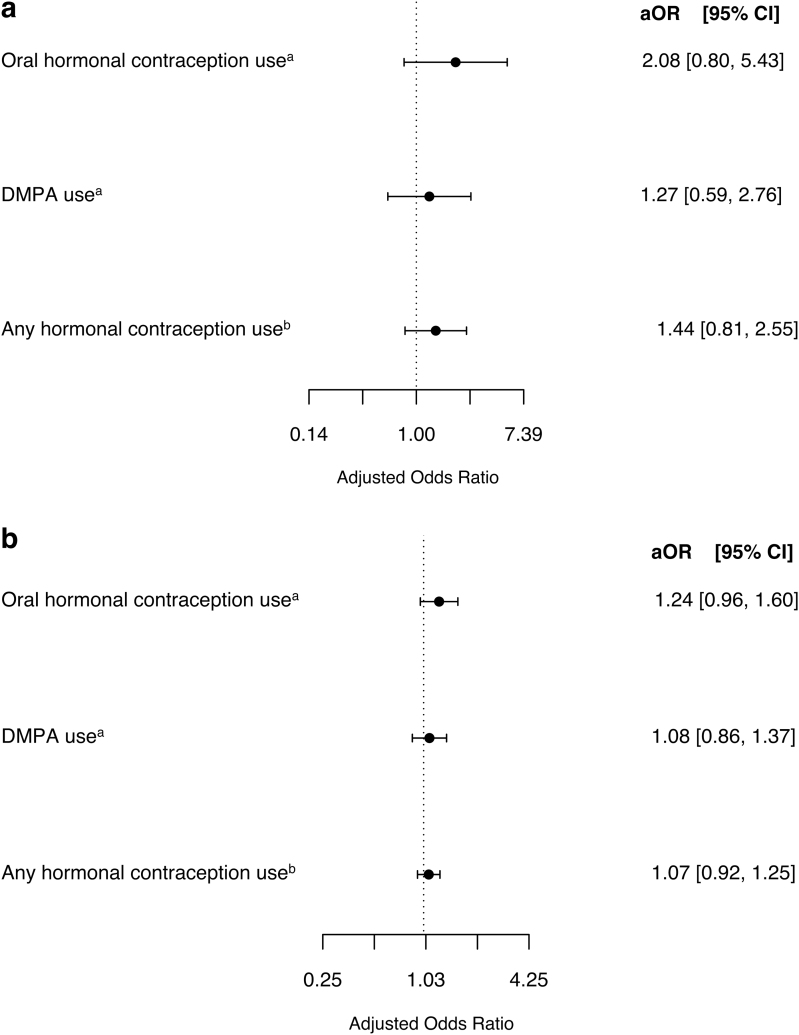
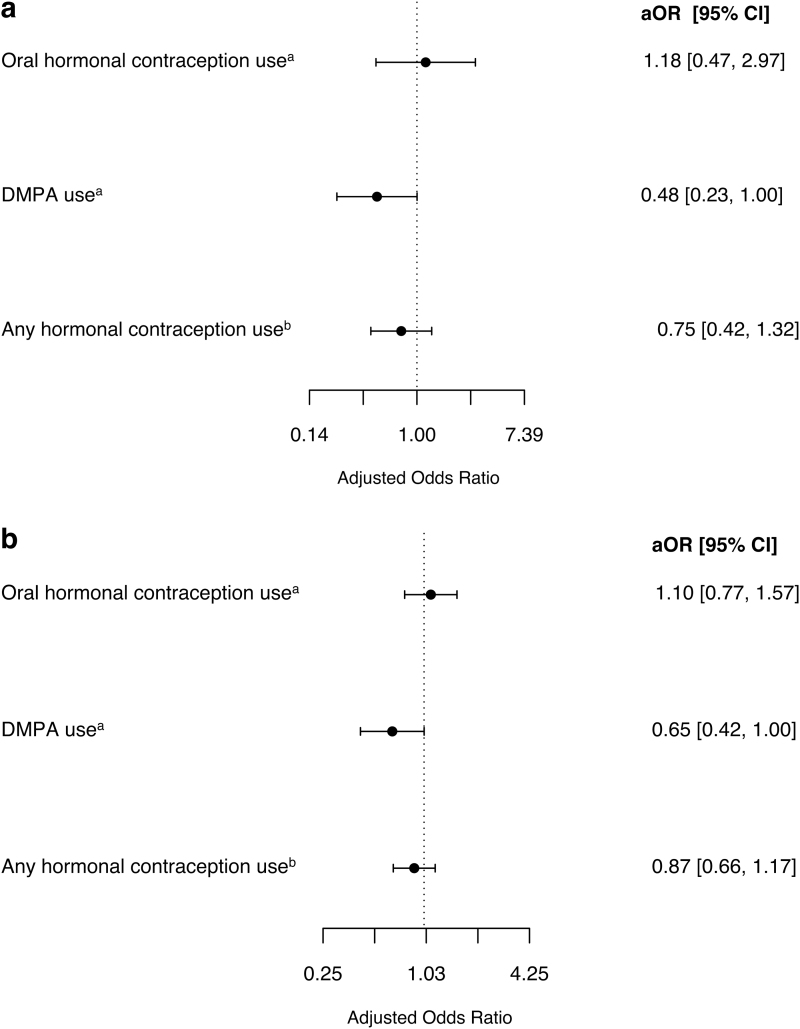
Objective: We sought to determine the association of hormonal contraception (HC) and cardiometabolic outcomes among women with human immunodeficiency virus (HIV). Methods: We included women with HIV aged 18-45 years in clinical care in the Southeastern United States between 1998 and 2018. Oral and injectable HC use was captured from medication records. Our outcomes included incident cardiovascular/thrombotic disease (CVD) (atherosclerosis, hypertension, cerebrovascular disease, thrombosis, and heart failure) and incident metabolic disorders (diabetes, dyslipidemia, obesity, and non-alcoholic steatohepatitis). We excluded women with prevalent conditions. We used multivariable marginal structural models to examine time-varying current and cumulative HC use and cardiometabolic outcomes in separate analyses, adjusting for age, race, smoking, time-varying comorbidities, CD4 cell count, HIV RNA, and antiretroviral use. Women with HC exposure were compared with women without HC exposure. Results: Among the 710 women included, 201 women (28%) used HC. CVD analyses included 603 women without prevalent CVD and 93 incident events; metabolic analyses included 365 women without prevalent metabolic disease and 150 incident events. Current and cumulative oral HC use was associated with increased odds of CVD, though this was not statistically significant (adjusted odds ratio [aOR] = 2.08, [95% confidence interval (CI): 0.80-5.43] and aOR = 1.24 [95% CI: 0.96-1.60] per year of use, respectively). Oral HC was not associated with risk of incident metabolic disorders. Depot medroxyprogesterone acetate (DMPA) was not associated with risk of incident CVD. Current and cumulative DMPA use was significantly associated with decreased odds of incident metabolic disorders (aOR = 0.48 [95% CI: 0.23, 1.00] and aOR = 0.65 [95% CI: 0.42-1.00] per year of use, respectively). Conclusion: Our results suggest that cardiovascular risk should be considered when selecting contraception for women with HIV.
Keywords: HIV; cardiometabolic disease; contraception; women.
Figures
Similar articles
-
Risk of thromboembolism in patients with COVID-19 who are using hormonal contraception.Cochrane Database Syst Rev. 2023 Jan 9;1(1):CD014908. doi: 10.1002/14651858.CD014908.pub2. Cochrane Database Syst Rev. 2023. Update in: Cochrane Database Syst Rev. 2023 May 15;5:CD014908. doi: 10.1002/14651858.CD014908.pub3. PMID: 36622724 Free PMC article. Updated.
-
Steroidal contraceptives and bone fractures in women: evidence from observational studies.Cochrane Database Syst Rev. 2012 Aug 15;(8):CD009849. doi: 10.1002/14651858.CD009849.pub2. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2015 Jul 21;(7):CD009849. doi: 10.1002/14651858.CD009849.pub3. PMID: 22895991 Updated.
-
Combined hormonal contraceptive use among women with known dyslipidemias: a systematic review of critical safety outcomes.Contraception. 2016 Sep;94(3):280-7. doi: 10.1016/j.contraception.2015.08.002. Epub 2015 Aug 10. Contraception. 2016. PMID: 26272309
-
Progestin-only contraceptives: effects on weight.Cochrane Database Syst Rev. 2016 Aug 28;2016(8):CD008815. doi: 10.1002/14651858.CD008815.pub4. Cochrane Database Syst Rev. 2016. PMID: 27567593 Free PMC article.
-
School-based interventions for improving contraceptive use in adolescents.Cochrane Database Syst Rev. 2016 Jun 29;2016(6):CD012249. doi: 10.1002/14651858.CD012249. Cochrane Database Syst Rev. 2016. PMID: 27353385 Free PMC article.
References
-
- CDC. HIV and Women. 2020. Available from: https://www.cdc.gov/hiv/group/gender/women/index.html [Last accessed: August 27, 2020].
-
- UNAIDS. The Gap Report; 2014; p. 135.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
