

Overview of Rheumatoid Arthritis-Associated Interstitial Lung Disease and Its Treatment
- PMID: 38484788
- PMCID: PMC11483238
- DOI: 10.1055/s-0044-1782218
Overview of Rheumatoid Arthritis-Associated Interstitial Lung Disease and Its Treatment
Abstract
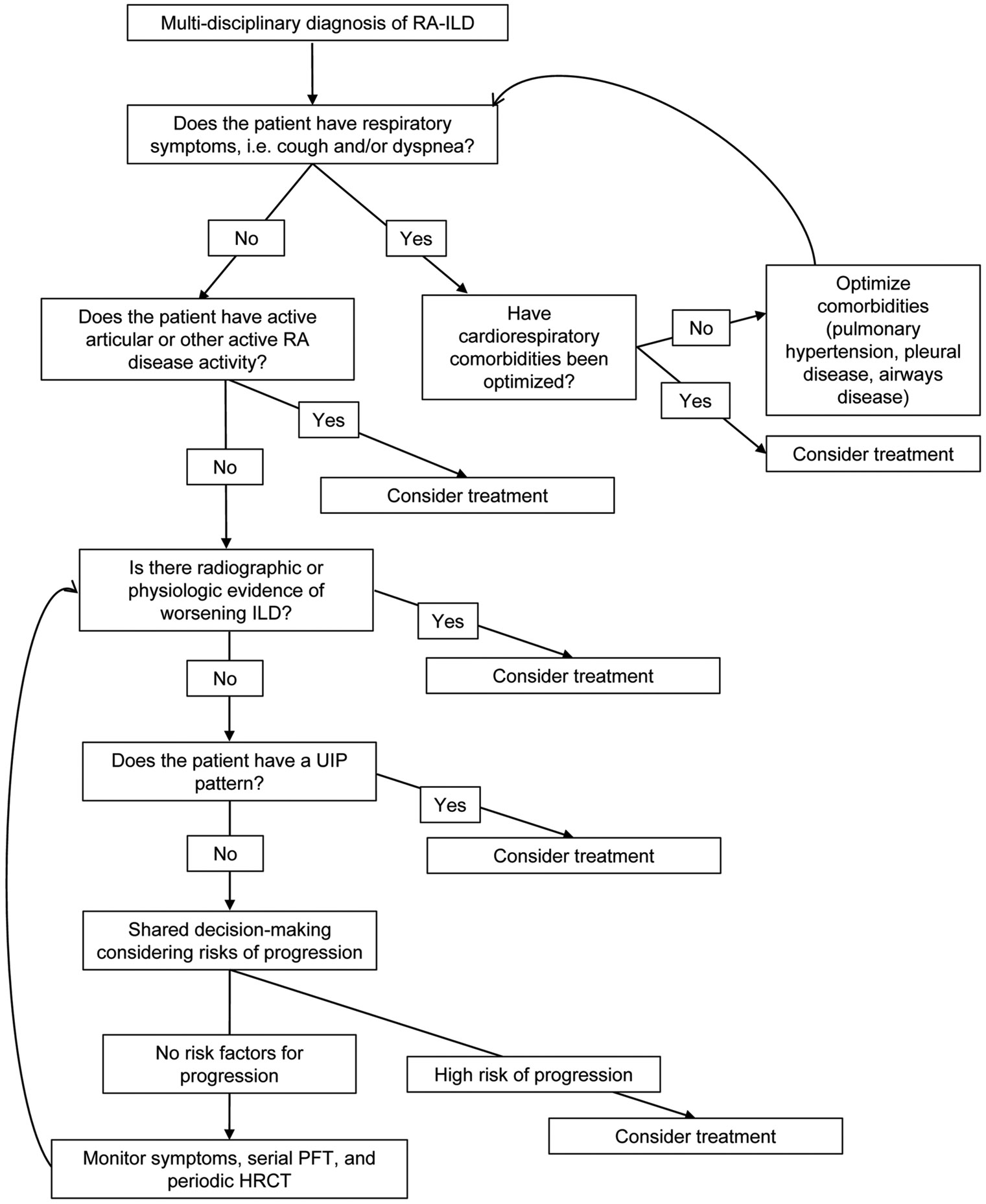
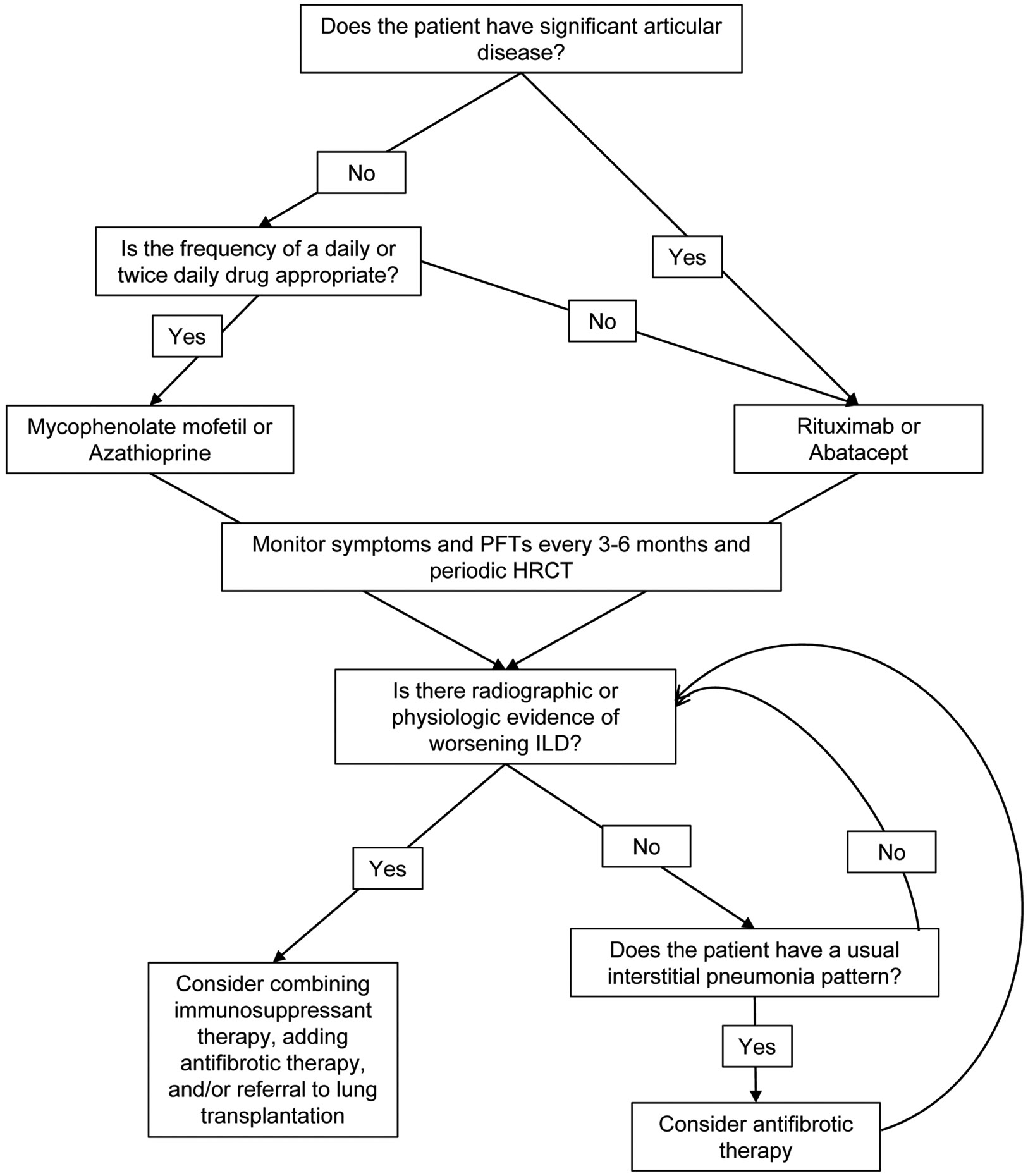
Interstitial lung disease (ILD) is a common pulmonary complication of rheumatoid arthritis (RA), causing significant morbidity and mortality. Optimal treatment for RA-ILD is not yet well defined. Reliable prognostic indicators are largely byproducts of prior ILD progression, including low or decreasing forced vital capacity and extensive or worsening fibrosis on imaging. In the absence of validated tools to predict treatment response, decisions about whether to initiate or augment treatment are instead based on clinical judgment. In general, treatment should be initiated in patients who are symptomatic, progressing, or at high risk of poor outcomes. Retrospective data suggest that mycophenolate mofetil, azathioprine, and rituximab are likely effective therapies for RA-ILD. Abatacept is also emerging as a potential first-line treatment option for patients with RA-ILD. Further, recent data demonstrate that immunosuppression may be beneficial even in patients with a usual interstitial pneumonia (UIP) pattern on imaging, suggesting that immunosuppression should be considered irrespective of imaging pattern. Recent randomized controlled trials have shown that antifibrotic medications, such as nintedanib and likely pirfenidone, slow forced vital capacity decline in RA-ILD. Consideration can be given to antifibrotic initiation in patients progressing despite immunosuppression, particularly in patients with a UIP pattern. Future research directions include developing tools to predict which patients will remain stable from patients who will progress, discriminating patients who will respond to treatment from nonresponders, and developing algorithms for starting immunosuppression, antifibrotics, or both as first-line therapies.
Thieme. All rights reserved.
Conflict of interest statement
J.V.P. reports no conflicts. J.S.L. reports receiving grants from the NIH and Boehringer Ingelheim, an unrestricted research gift from Pliant, and consulting fees from Blade, Boehringer Ingelheim, United Therapeutics, AstraZeneca, and Eleven P15, outside the submitted work. J.S.L. is/has been on the DSMB for United Therapeutics and Avalyn and is an advisor for the Pulmonary Fibrosis Foundation, outside the submitted work.
Figures
Similar articles
-
Treatment Outcomes for Rheumatoid Arthritis-Associated Interstitial Lung Disease: A Real-World, Multisite Study of the Impact of Immunosuppression on Pulmonary Function Trajectory.Chest. 2023 Apr;163(4):861-869. doi: 10.1016/j.chest.2022.11.035. Epub 2022 Dec 5. Chest. 2023. PMID: 36470416 Free PMC article. Clinical Trial.
-
Antifibrotics in rheumatoid arthritis-associated interstitial lung disease - real-world data from a nationwide cohort.ARP Rheumatol. 2024 Jul-Sep;3(3):182-188. doi: 10.63032/POPM9413. ARP Rheumatol. 2024. PMID: 39368099 English.
-
Recent advances in rheumatoid arthritis-associated interstitial lung disease.Curr Opin Pulm Med. 2020 Sep;26(5):477-486. doi: 10.1097/MCP.0000000000000710. Curr Opin Pulm Med. 2020. PMID: 32701675 Review.
-
Evaluation and management of rheumatoid arthritis-associated interstitial lung disease.Respir Investig. 2025 Jul;63(4):699-710. doi: 10.1016/j.resinv.2025.05.011. Epub 2025 Jun 5. Respir Investig. 2025. PMID: 40479958 Review.
-
Real-world evidence of the antifibrotic nintedanib in rheumatoid arthritis-interstitial lung disease. National multicenter study of 74 patients.Semin Arthritis Rheum. 2025 Jun;72:152710. doi: 10.1016/j.semarthrit.2025.152710. Epub 2025 Mar 14. Semin Arthritis Rheum. 2025. PMID: 40117729
Cited by
-
Rituximab, Apremilast, and Upadacitinib as Selected Biosimilar and Targeted Synthetic Disease-Modifying Antirheumatic Drugs with Diverse Mechanisms of Action: Their Current Use in Slowing Down the Progression of Disease.J Clin Med. 2025 Apr 10;14(8):2605. doi: 10.3390/jcm14082605. J Clin Med. 2025. PMID: 40283434 Free PMC article. Review.
-
Patient-Centric Approach for the Treatment of Rheumatoid Arthritis-Associated Interstitial Lung Disease in Older People.Drugs Aging. 2025 Feb;42(2):81-94. doi: 10.1007/s40266-024-01175-0. Epub 2025 Jan 13. Drugs Aging. 2025. PMID: 39800810 Review.
-
Interstitial Lung Disease Associated with Anti-Ku Antibodies: A Case Series of 19 Patients.J Clin Med. 2025 Jan 3;14(1):247. doi: 10.3390/jcm14010247. J Clin Med. 2025. PMID: 39797328 Free PMC article.
-
From Gut to Lung: The Role of Bile Acids in Rheumatoid Arthritis-Associated Interstitial Lung Disease (RA-ILD).J Inflamm Res. 2025 Aug 2;18:10331-10340. doi: 10.2147/JIR.S524111. eCollection 2025. J Inflamm Res. 2025. PMID: 40778337 Free PMC article. Review.
-
A noval identification of 4 systemic sclerosis - interstitial lung disease subgroups using principal component analysis-based cluster analysis.BMC Pulm Med. 2025 May 21;25(1):248. doi: 10.1186/s12890-025-03722-w. BMC Pulm Med. 2025. PMID: 40399864 Free PMC article.
References
-
- Safiri S, Kolahi AA, Hoy D, et al. Global, regional and national burden of rheumatoid arthritis 1990-2017: a systematic analysis of the Global Burden of Disease study 2017. Ann Rheum Dis 2019;78(11):1463–1471 - PubMed
-
- England BR, Sayles H, Michaud K, et al. Cause-specific mortality in male US Veterans with rheumatoid arthritis. Arthritis Care Res (Hoboken) 2016;68(01):36–45 - PubMed
-
- Hayakawa H, Sato A, Imokawa S, Toyoshima M, Chida K, Iwata M. Bronchiolar disease in rheumatoid arthritis. Am J Respir Crit Care Med 1996;154(05):1531–1536 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical