

Optic Nerve Sheath MR Imaging Measurements in Patients with Orthostatic Headaches and Normal Findings on Conventional Imaging Predict the Presence of an Underlying CSF-Venous Fistula
- PMID: 38485201
- PMCID: PMC11288531
- DOI: 10.3174/ajnr.A8165
Optic Nerve Sheath MR Imaging Measurements in Patients with Orthostatic Headaches and Normal Findings on Conventional Imaging Predict the Presence of an Underlying CSF-Venous Fistula
Abstract
Background and purpose: Spontaneous spinal CSF leaks typically cause orthostatic headache, but their detection may require specialized and invasive spinal imaging. We undertook a study to determine the value of simple optic nerve sheath MR imaging measurements in predicting the likelihood of finding a CSF-venous fistula, a type of leak that cannot be detected with routine spine MR imaging or CT myelography, among patients with orthostatic headache and normal conventional brain and spine imaging findings.
Materials and methods: This cohort study included a consecutive group of patients with orthostatic headache and normal conventional brain and spine imaging findings who underwent digital subtraction myelography under general anesthesia to look for spinal CSF-venous fistulas.
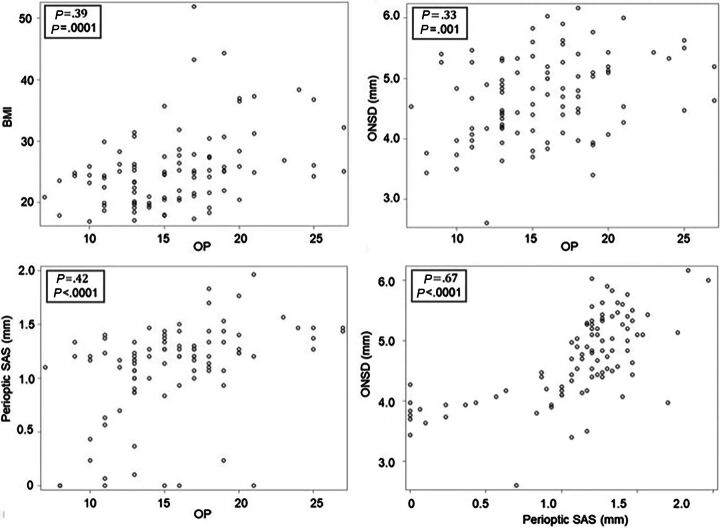
Results: The study group consisted of 93 patients (71 women and 22 men; mean age, 47.5 years; range, 17-84 years). Digital subtraction myelography demonstrated a CSF-venous fistula in 15 patients. The mean age of these 8 women and 7 men was 56 years (range, 23-83 years). The mean optic nerve sheath diameter was 4.0 mm, and the mean perioptic subarachnoid space was 0.5 mm in patients with a CSF-venous fistula compared with 4.9 and 1.2 mm, respectively, in patients without a fistula (P < .001). Optimal cutoff values were found at 4.4 mm for optic nerve sheath diameter and 1.0 mm for the perioptic subarachnoid space. Fistulas were detected in about 50% of patients with optic nerve sheath diameter or perioptic subarachnoid space measurements below these cutoff values compared with <2% of patients with optic nerve sheath diameter or perioptic subarachnoid space measurements above these cutoff values. Following surgical ligation of the fistula, optic nerve sheath diameter increased from 4.0 to 5.3 mm and the perioptic subarachnoid space increased from 0.5 to 1.2 mm (P < .001).
Conclusions: Concerns about a spinal CSF leak should not be dismissed in patients with orthostatic headache when conventional imaging findings are normal, and simple optic nerve sheath MR imaging measurements can help decide if more imaging needs to be performed in this patient population.
© 2024 by American Journal of Neuroradiology.
Figures




References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical