

PTCy versus ATG as graft-versus-host disease prophylaxis in mismatched unrelated stem cell transplantation
- PMID: 38485723
- PMCID: PMC10940681
- DOI: 10.1038/s41408-024-01032-8
PTCy versus ATG as graft-versus-host disease prophylaxis in mismatched unrelated stem cell transplantation
Abstract
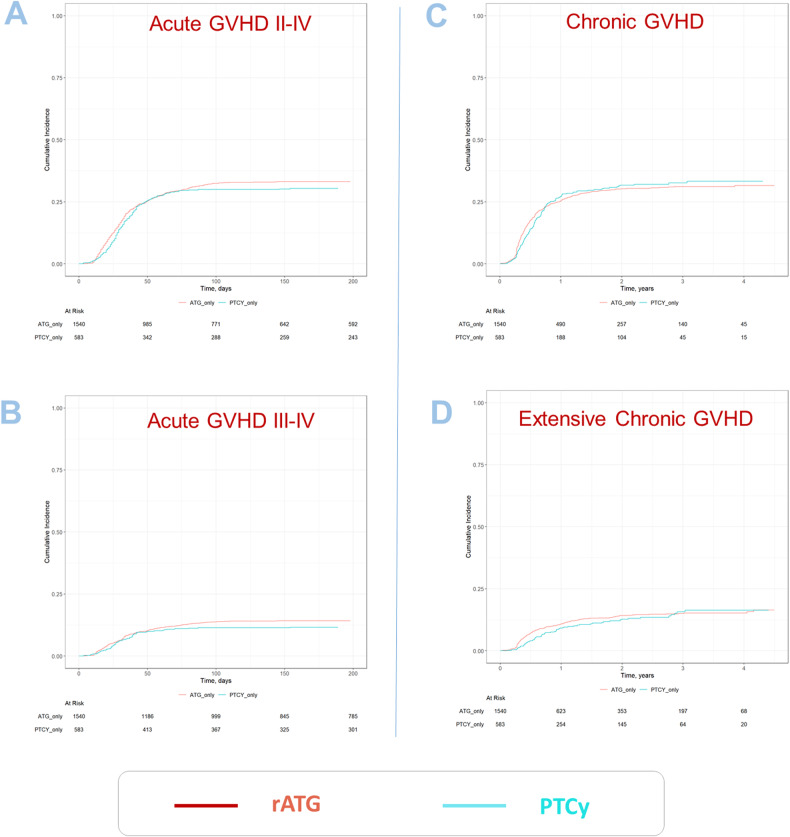
There is an increased risk of GVHD and of non-relapse mortality (NRM) after allogeneic stem cell transplantations (alloSCT) when mismatched unrelated donors (MMUD) are used. In Europe, it is standard practice to use rabbit anti-thymocyte globulin (rATG) to reduce the high NRM and GVHD risks after MMUD alloSCT. As an alternative to rATG, post-transplantation Cyclophosphamide (PTCy) is in increasing clinical use. It is currently impossible to give general recommendations regarding preference for one method over another since comparative evidence from larger data sets is lacking. To improve the evidence base, we analyzed the outcome of rATG vs. PTCy prophylaxis in adult patients with hematologic malignancies undergoing first peripheral blood alloSCT from MMUD (9/10 antigen match) between Jan 2018 and June 2021 in the database of the European Society for Blood and Marrow Transplantation (EBMT). We performed multivariate analyses using the Cox proportional-hazards regression model. We included 2123 patients in the final analyses (PTCy, n = 583; rATG, n = 1540). p values and hazard ratios (HR) presented here are multivariate outcomes. Two years after alloSCT we found a lower NRM in the PTCy group of 18% vs. 24.9% in the rATG group; p = 0.028, HR 0.74. Overall survival in the PTCy cohort was higher with 65.7% vs. 55.7% in the rATG cohort; p < 0.001, HR 0.77. Progression-free survival was also better in the PTCy patients with 59.1% vs. 48.8% when using rATG; p = 0.001, 0.78. The incidences of chronic GVHD and acute GVHD were not significantly different between the groups. We found significantly lower NRM as well as higher survival in recipients of peripheral blood alloSCTs from MMUD receiving PTCy as compared to rATG. The results of the current analysis suggest an added value of PTCy as GVHD prophylaxis in MMUD alloSCT.
© 2024. The Author(s).
Conflict of interest statement
OP has received honoraria or travel support from Gilead, Jazz, MSD, Novartis, Pfizer and Therakos. He has received research support from Incyte and Priothera. He is member of advisory boards to Equillium Bio, Jazz, Gilead, Novartis, MSD, Omeros, Priothera, Sanofi, Shionogi and SOBI. HS reports having received personal fees from Incyte, Janssen, Novartis, Sanofi and from the Belgian Hematological Society (BHS), as well as research grants from Novartis and the BHS, all paid to her institution. She has also received non-financial support from Gilead, Pfizer, the EBMT (European Society for Blood and Marrow transplantation) and the CIBMTR (Center for International Bone Marrow Transplantation Research). IM received honoraria or travel support from Novartis, Sanofi, SOBI, Takeda. CCL received honoraria or travel support from Gilead/Kite and Therakos. Consulting fees for advisory board from Gilead/Kite, Nektar Therapeutics. FB participated to AB and received speaker fees from NEOVII and SANOFI. PD reports consultancy for AbbVie, AstraZeneca, Beigene, BMS, Gilead, Miltenyi, Novartis, Riemser; speakers bureau for AbbVie, AstraZeneca, BeiGene, BMS, Gilead, Novartis, Riemser, Roche; research support from Riemser (all to institution).
Figures

References
-
- Saraceni F, Labopin M, Gorin NC, Blaise D, Tabrizi R, Volin L, et al. Matched and mismatched unrelated donor compared to autologous stem cell transplantation for acute myeloid leukemia in first complete remission: a retrospective, propensity score-weighted analysis from the ALWP of the EBMT. J Hematol Oncol. 2016;9:79. doi: 10.1186/s13045-016-0314-x. - DOI - PMC - PubMed
-
- Bolanos-Meade J, Reshef R, Fraser R, Fei M, Abhyankar S, Al-Kadhimi Z, et al. Three prophylaxis regimens (tacrolimus, mycophenolate mofetil, and cyclophosphamide; tacrolimus, methotrexate, and bortezomib; or tacrolimus, methotrexate, and maraviroc) versus tacrolimus and methotrexate for prevention of graft-versus-host disease with haemopoietic cell transplantation with reduced-intensity conditioning: a randomised phase 2 trial with a non-randomised contemporaneous control group (BMT CTN 1203) Lancet Haematol. 2019;6:e132–43. doi: 10.1016/S2352-3026(18)30221-7. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
