Identification of a hyperinflammatory sepsis phenotype using protein biomarker and clinical data in the ProCESS randomized trial
- PMID: 38485953
- PMCID: PMC10940677
- DOI: 10.1038/s41598-024-55667-5
Identification of a hyperinflammatory sepsis phenotype using protein biomarker and clinical data in the ProCESS randomized trial
Abstract
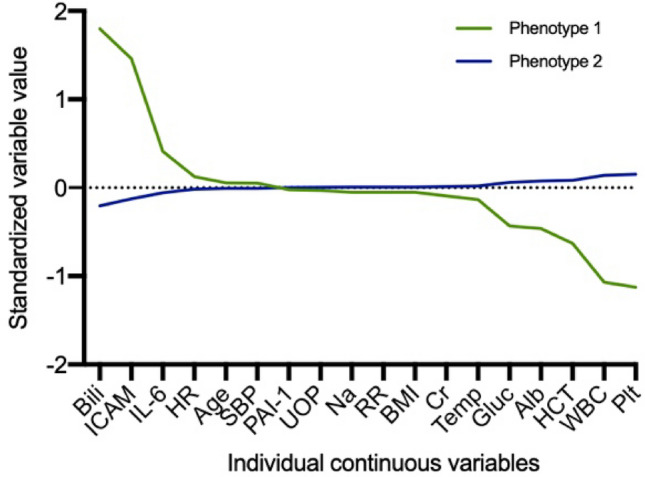
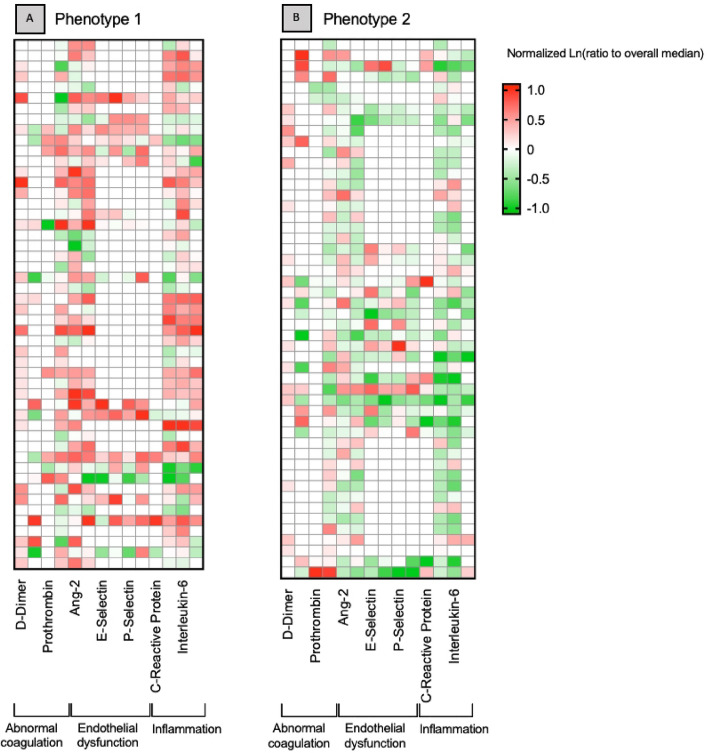
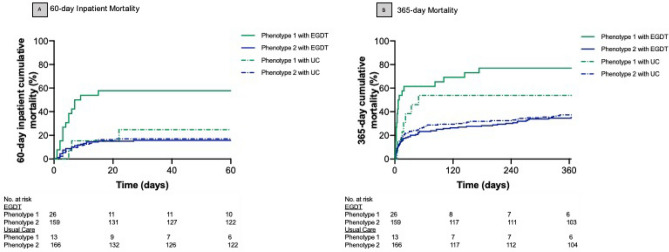
Sepsis is a heterogeneous syndrome and phenotypes have been proposed using clinical data. Less is known about the contribution of protein biomarkers to clinical sepsis phenotypes and their importance for treatment effects in randomized trials of resuscitation. The objective is to use both clinical and biomarker data in the Protocol-Based Care for Early Septic Shock (ProCESS) randomized trial to determine sepsis phenotypes and to test for heterogeneity of treatment effect by phenotype comparing usual care to protocolized early, goal-directed therapy(EGDT). In this secondary analysis of a subset of patients with biomarker sampling in the ProCESS trial (n = 543), we identified sepsis phenotypes prior to randomization using latent class analysis of 20 clinical and biomarker variables. Logistic regression was used to test for interaction between phenotype and treatment arm for 60-day inpatient mortality. Among 543 patients with severe sepsis or septic shock in the ProCESS trial, a 2-class model best fit the data (p = 0.01). Phenotype 1 (n = 66, 12%) had increased IL-6, ICAM, and total bilirubin and decreased platelets compared to phenotype 2 (n = 477, 88%, p < 0.01 for all). Phenotype 1 had greater 60-day inpatient mortality compared to Phenotype 2 (41% vs 16%; p < 0.01). Treatment with EGDT was associated with worse 60-day inpatient mortality compared to usual care (58% vs. 23%) in Phenotype 1 only (p-value for interaction = 0.05). The 60-day inpatient mortality was similar comparing EGDT to usual care in Phenotype 2 (16% vs. 17%). We identified 2 sepsis phenotypes using latent class analysis of clinical and protein biomarker data at randomization in the ProCESS trial. Phenotype 1 had increased inflammation, organ dysfunction and worse clinical outcomes compared to phenotype 2. Response to EGDT versus usual care differed by phenotype.
Keywords: Biomarkers; Phenotypes; Sepsis.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures