

Italian guidelines for the management of irritable bowel syndrome in children and adolescents : Joint Consensus from the Italian Societies of: Gastroenterology, Hepatology and Pediatric Nutrition (SIGENP), Pediatrics (SIP), Gastroenterology and Endoscopy (SIGE) and Neurogastroenterology and Motility (SINGEM)
- PMID: 38486305
- PMCID: PMC10938778
- DOI: 10.1186/s13052-024-01607-y
Italian guidelines for the management of irritable bowel syndrome in children and adolescents : Joint Consensus from the Italian Societies of: Gastroenterology, Hepatology and Pediatric Nutrition (SIGENP), Pediatrics (SIP), Gastroenterology and Endoscopy (SIGE) and Neurogastroenterology and Motility (SINGEM)
Abstract
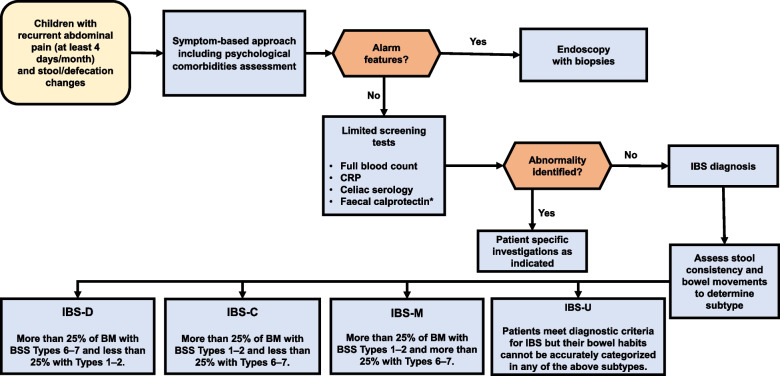
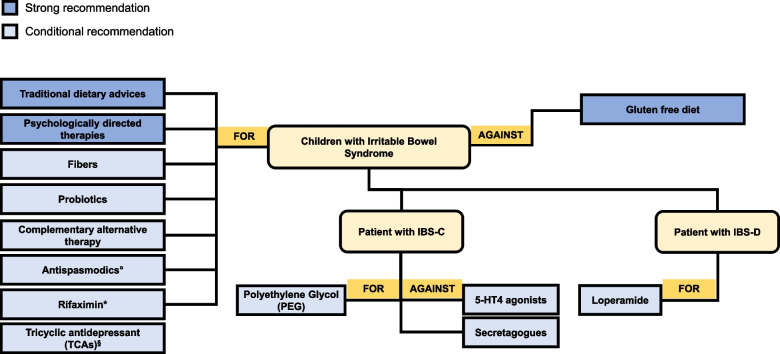
The irritable bowel syndrome (IBS) is a functional gastrointestinal disorder (FGID), whose prevalence has widely increased in pediatric population during the past two decades. The exact pathophysiological mechanism underlying IBS is still uncertain, thus resulting in challenging diagnosis and management. Experts from 4 Italian Societies participated in a Delphi consensus, searching medical literature and voting process on 22 statements on both diagnosis and management of IBS in children. Recommendations and levels of evidence were evaluated according to the grading of recommendations, assessment, development, and evaluation (GRADE) criteria. Consensus was reached for all statements. These guidelines suggest a positive diagnostic strategy within a symptom-based approach, comprehensive of psychological comorbidities assessment, alarm signs and symptoms' exclusion, testing for celiac disease and, under specific circumstances, fecal calprotectin and C-reactive protein. Consensus also suggests to rule out constipation in case of therapeutic failure. Conversely, routine stool testing for enteric pathogens, testing for food allergy/intolerance or small intestinal bacterial overgrowth are not recommended. Colonoscopy is recommended only in patients with alarm features. Regarding treatment, the consensus strongly suggests a dietary approach, psychologically directed therapies and, in specific conditions, gut-brain neuromodulators, under specialist supervision. Conditional recommendation was provided for both probiotics and specific fibers supplementation. Polyethylene glycol achieved consensus recommendation for specific subtypes of IBS. Secretagogues and 5-HT4 agonists are not recommended in children with IBS-C. Certain complementary alternative therapies, antispasmodics and, in specific IBS subtypes, loperamide and rifaximin could be considered.
Keywords: Children; Chronic abdominal pain; Constipation; Diarrhea; Functional gastrointestinal disorders; Irritable bowel syndrome.
© 2024. The Author(s).
Conflict of interest statement
The following authors declare the following paid or unpaid consultancies, business interests or sources of honoraria payments for the past three years, and anything else which could potentially be viewed as a conflict of interest:
GB: Aboca, AB Biotics, Agave, Alfa Sigma, AGPharma, Bayer, Bromatech, Cadigroup, Biocodex, Sanofi, GE Healthcare, Mayoly, Diadema, Sofar;
CC: Sofar, Interalia Pharma, Schwabe Pharma; consultation fees from Alfa Sigma;
AS: is clinical investigator for Janssen Biologics B.V., Eli Lilly Cork Limited and Novalac; consultant for Aboca, Abbott, Angelini e Novalac; was clinical investigator for Aboca and PAREXEL International.
VS: Alfa Sigma, Bayer, Coloplast, GE Healthcare, Menarini, Norgine.
All the other authors declared no conflicts of interest.
Figures
References
-
- Hyams JS, Di Lorenzo C, Saps M, Shulman RJ, Staiano A, van Tilburg M. Functional disorders: children and adolescents. Gastroenterology. 2016;S0016–5085(16):00181–185. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
