

Artificial intelligence-based MRI radiomics and radiogenomics in glioma
- PMID: 38486342
- PMCID: PMC10938723
- DOI: 10.1186/s40644-024-00682-y
Artificial intelligence-based MRI radiomics and radiogenomics in glioma
Abstract
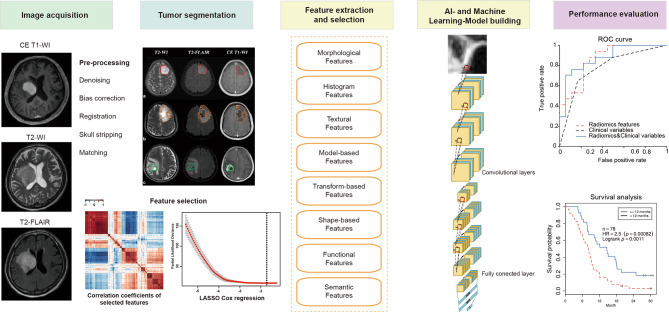
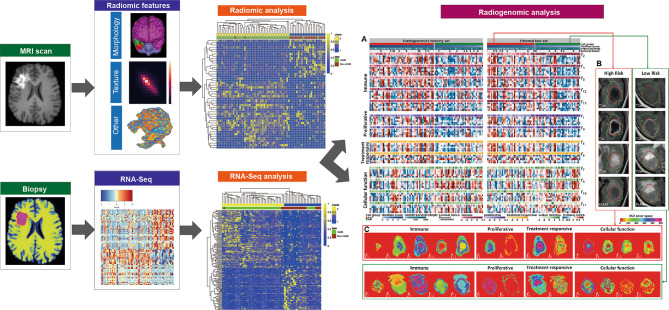
The specific genetic subtypes that gliomas exhibit result in variable clinical courses and the need to involve multidisciplinary teams of neurologists, epileptologists, neurooncologists and neurosurgeons. Currently, the diagnosis of gliomas pivots mainly around the preliminary radiological findings and the subsequent definitive surgical diagnosis (via surgical sampling). Radiomics and radiogenomics present a potential to precisely diagnose and predict survival and treatment responses, via morphological, textural, and functional features derived from MRI data, as well as genomic data. In spite of their advantages, it is still lacking standardized processes of feature extraction and analysis methodology among different research groups, which have made external validations infeasible. Radiomics and radiogenomics can be used to better understand the genomic basis of gliomas, such as tumor spatial heterogeneity, treatment response, molecular classifications and tumor microenvironment immune infiltration. These novel techniques have also been used to predict histological features, grade or even overall survival in gliomas. In this review, workflows of radiomics and radiogenomics are elucidated, with recent research on machine learning or artificial intelligence in glioma.
Keywords: Artificial intelligence; Glioma; MRI; Machine learning; Radiogenomics; Radiomics.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
