

Clinical impact of the Kidney Failure Risk Equation for vascular access planning
- PMID: 38486367
- PMCID: PMC11648961
- DOI: 10.1093/ndt/gfae064
Clinical impact of the Kidney Failure Risk Equation for vascular access planning
Abstract
Background: Risk-based thresholds for arteriovenous (AV) access creation has been proposed to aid vascular access planning. We aimed to assess the clinical impact of implementing the Kidney Failure Risk Equation (KFRE) for vascular access referral.
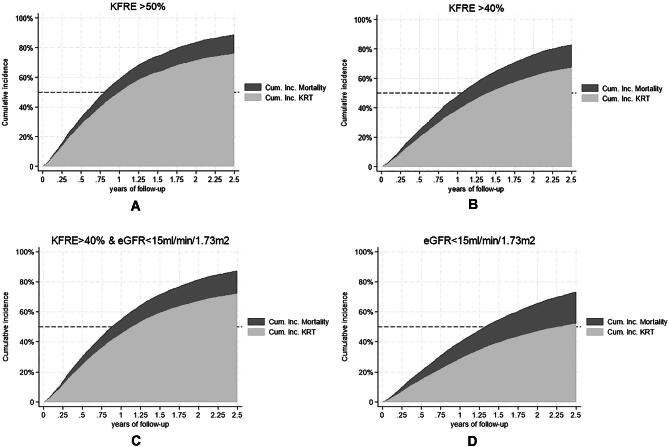
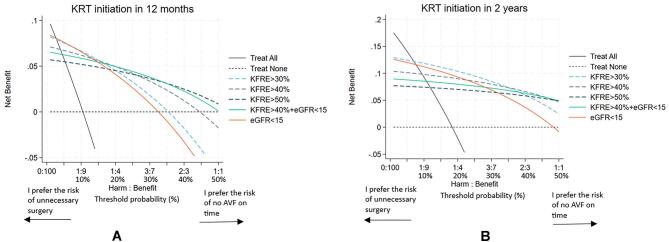
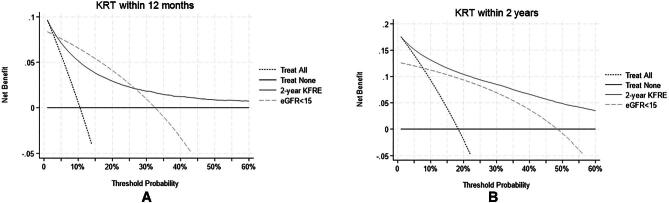
Methods: A total of 16 102 nephrology-referred chronic kidney disease (CKD) patients from the Swedish Renal Registry 2008-18 were included. The KFRE was calculated repeatedly, and the timing was identified for when the KFRE risk exceeded several pre-defined thresholds and/or the estimated glomerular filtration rate was <15 mL/min/1.73 m2 (eGFR15). To assess the utility of the KFRE/eGFR thresholds, cumulative incidence curves of kidney replacement therapy (KRT) or death, and decision-curve analyses were computed at 6 and 12 months, and 2 years. The potential impact of using the different thresholds was illustrated by an example from the Swedish access registry.
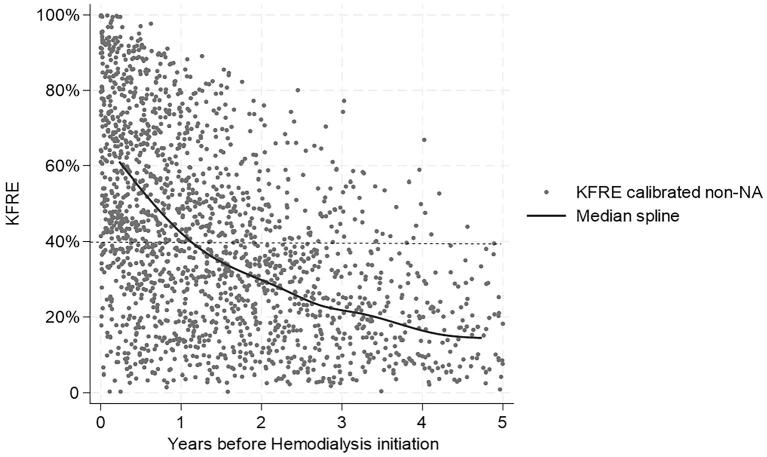
Results: The 12-month specificity for KRT initiation was highest for KFRE >50% {94.5 [95% confidence interval (CI) 94.3-94.7]} followed by KFRE >40% [90.0 (95% CI 89.7-90.3)], while sensitivity was highest for KFRE >30% [79.3 (95% CI 78.2-80.3)] and eGFR <15 mL/min/1.73 m2 [81.2 (95% CI 80.2-82.2)]. The 2-year positive predictive value was 71.5 (95% CI 70.2-72.8), 61.7 (95% CI 60.4-63.0) and 47.2 (95% CI 46.1-48.3) for KFRE >50%, KFRE >40% and eGFR <15, respectively. Decision curve analyses suggested the largest net benefit for KFRE >40% over 2 years and KFRE >50% over 12 months when it is important to avoid the harm of possibly unnecessary surgery. In Sweden, 54% of nephrology-referred patients started hemodialysis in a central venous catheter (CVC), of whom only 5% had AV access surgery >6 months before initiation. Sixty percent of the CVC patients exceeded KFRE >40% a median of 0.8 years (interquartile range 0.4-1.5) before KRT initiation.
Conclusions: The utility of using KFRE >40% and KFRE >50% is higher compared with the more traditionally used eGFR threshold <15 mL/min/1.73 m2 for vascular access planning.
Keywords: CKD; arteriovenous fistula; epidemiology; haemodialysis; vascular access.
© The Author(s) 2024. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
None of the authors has any financial disclosures to declare in relation to the work submitted. M.E. reports payment for lectures by Astellas Pharma, AstraZeneca, Vifor Pharma, Fresenius Medical Care and Baxter Healthcare, and participation in advisory boards for Astellas Pharma, AstraZeneca and Vifor Pharma. U.H.L. reports speaker and consultancy engagements from Baxter Healthcare and Fresenius Medical Care.
Figures
References
-
- Crooks PW, Thomas CO, Compton-Phillips Aet al. Clinical outcomes and healthcare use associated with optimal ESRD starts. Am J Manag Care 2018;24:e305–11. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
