

Bioavailability of three novel oral, sustained-release pellets, relative to an immediate-release tablet containing 500 mg flucytosine: A randomized, open-label, crossover study in healthy volunteers
- PMID: 38488418
- PMCID: PMC10941517
- DOI: 10.1111/cts.13756
Bioavailability of three novel oral, sustained-release pellets, relative to an immediate-release tablet containing 500 mg flucytosine: A randomized, open-label, crossover study in healthy volunteers
Abstract
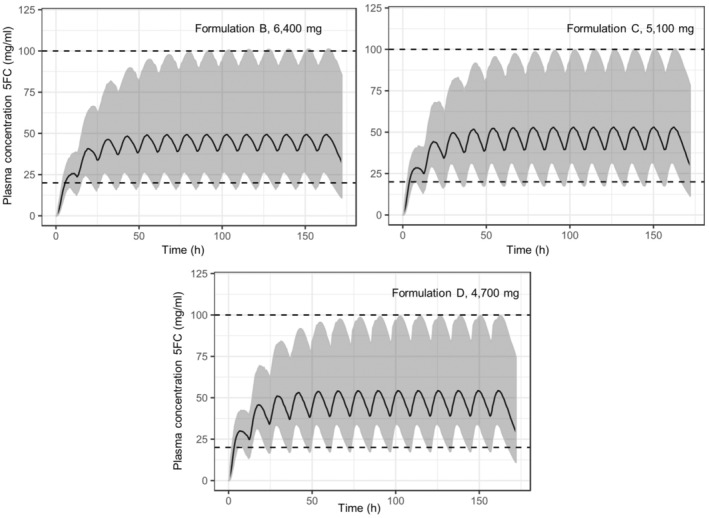
The opportunistic fungal infection cryptococcal meningoencephalitis is a major cause of death among people living with HIV in sub-Saharan Africa. We report pharmacokinetic (PK) and safety data from a randomized, four-period crossover phase I trial of three sustained-release (SR) oral pellet formulations of 5-flucytosine conducted in South Africa. These formulations were developed to require less frequent administration, to provide a convenient alternative to the current immediate release (IR) formulation, A. Formulations B, C, and D were designed to release 5-flucytosine as a percentage of the nominal dose in vitro. We assessed their safety and PK profiles in a single dose (1 × 3000 mg at 0 h), relative to commercial IR tablets (Ancotil 500 mg tablets; 3 × 500 mg at 0 h and 3 × 500 mg at 6 h) in healthy, fasted participants. Forty-two healthy participants were included. All treatments were well-tolerated. The primary PK parameters, maximum observed plasma concentration (Cmax ) and area under the concentration-time profiles, were significantly lower for the SR formulations than for the IR tablets, and the geometric mean ratios fell outside the conventional bioequivalence limits. The median maximum time to Cmax was delayed for the SR pellets. Physiologically-based PK modeling indicated a twice-daily 6400 mg dose of SR formulation D in fasted condition would be optimal for further clinical development. This regimen is predicted to result in a rapid steady-state plasma exposure with effective and safe trough plasma concentration and Cmax values, within the therapeutic boundaries relative to plasma exposure after four times per day administration of IR tablets (PACTR202201760181404).
© 2024 DNDI. Luxembourg Institute of Health. Pharmetheus AB. Mylan Laboratories Ltd. FARMOVS (Pty) Ltd and The Authors. Clinical and Translational Science published by Wiley Periodicals LLC on behalf of American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
The authors declared no competing interests for this work.
Figures



References
-
- World Health Organization . Guidelines for diagnosing, preventing and managing cryptococcal disease among adults, adolescents and children living with HIV. https://www.who.int/publications/i/item/9789240052178. Accessed March 21, 2023. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
