

Multiple surgical resections for progressive IDH wildtype glioblastoma-is it beneficial?
- PMID: 38488994
- PMCID: PMC10943163
- DOI: 10.1007/s00701-024-06025-x
Multiple surgical resections for progressive IDH wildtype glioblastoma-is it beneficial?
Abstract
Purpose: The role of repeat resection for recurrent glioblastoma (rGB) remains equivocal. This study aims to assess the overall survival and complications rates of single or repeat resection for rGB.
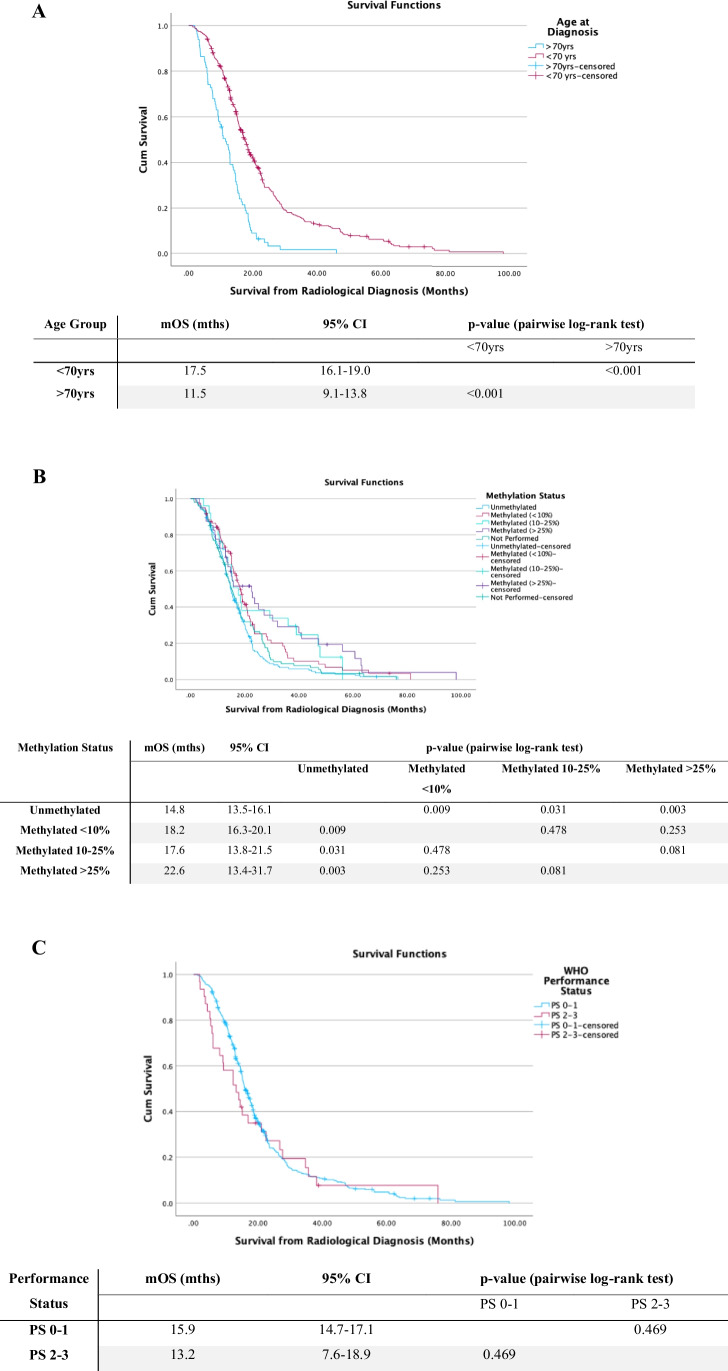
Methods: A single-centre retrospective review of all patients with IDH-wildtype glioblastoma managed surgically, between January 2014 and January 2022, was carried out. Patient survival and factors influencing prognosis were analysed, using Kaplan-Meier and Cox regression methods.
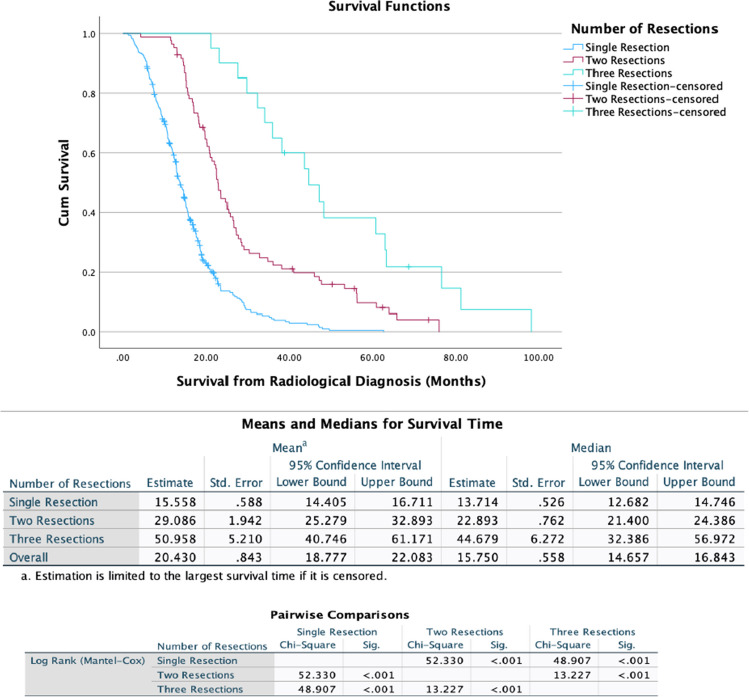
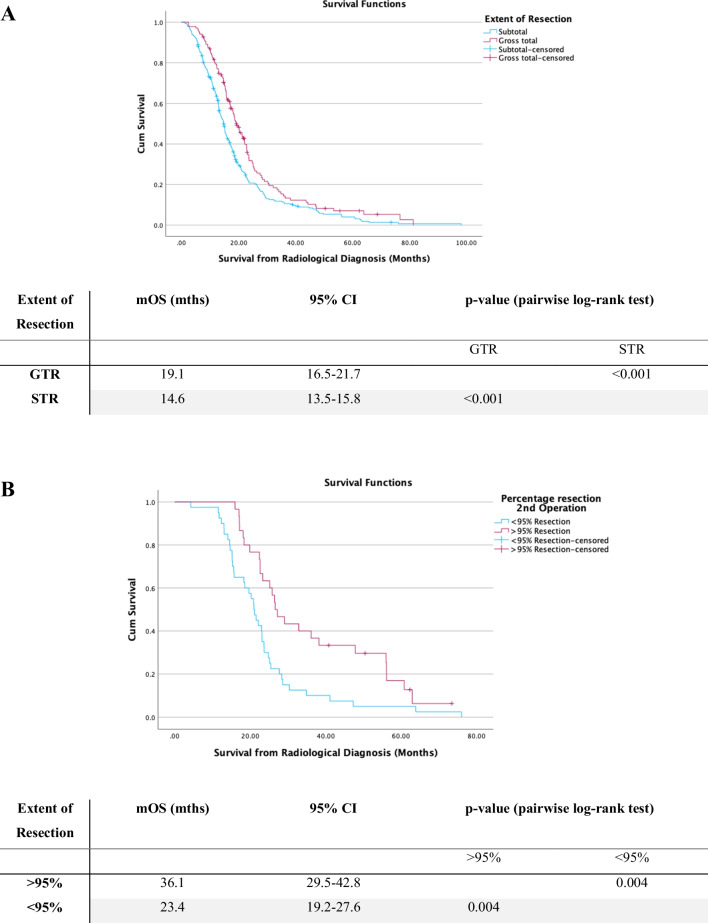
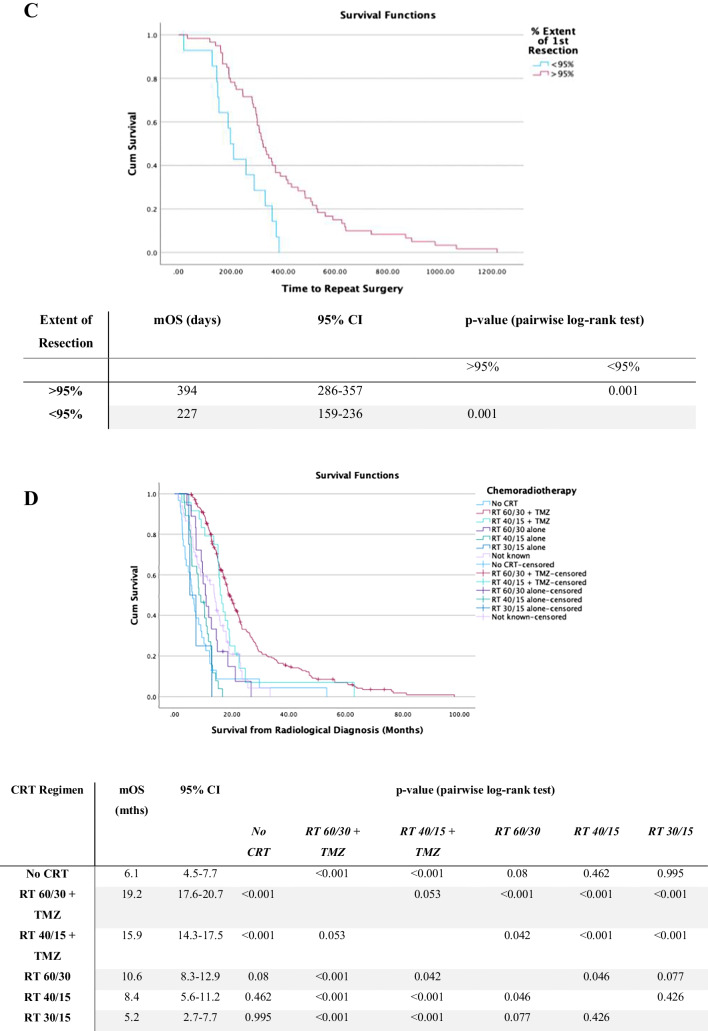
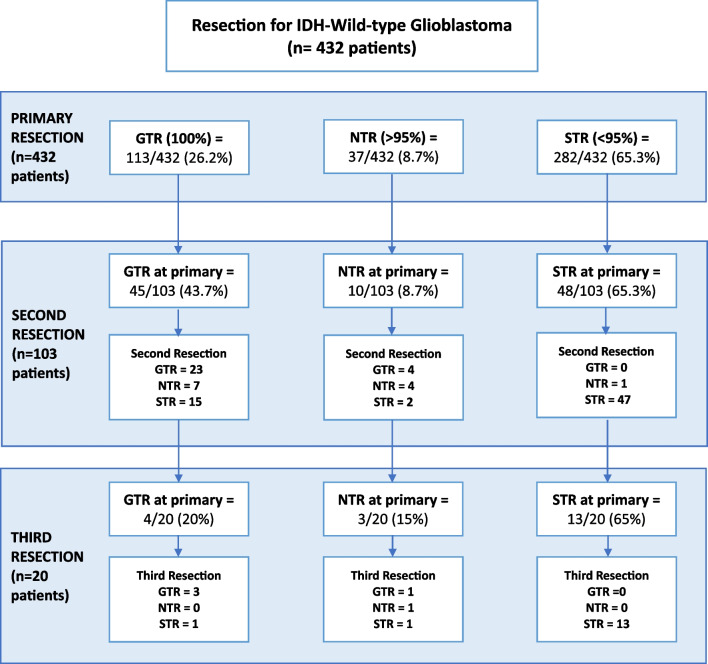
Results: Four hundred thirty-two patients were included, of whom 329 underwent single resection, 83 had two resections and 20 patients underwent three resections. Median OS (mOS) in the cohort who underwent a single operation was 13.7 months (95% CI: 12.7-14.7 months). The mOS was observed to be extended in patients who underwent second or third-time resection, at 22.9 months and 44.7 months respectively (p < 0.001). On second operation achieving > 95% resection or residual tumour volume of < 2.25 cc was significantly associated with prolonged survival. There was no significant difference in overall complication rates between primary versus second (p = 0.973) or third-time resections (p = 0.312). The use of diffusion tensor imaging (DTI) guided resection was associated with reduced post-operative neurological deficit (RR 0.37, p = 0.002), as was use of intraoperative ultrasound (iUSS) (RR 0.45, p = 0.04).
Conclusions: This study demonstrates potential prolongation of survival for rGB patients undergoing repeat resection, without significant increase in complication rates with repeat resections. Achieving a more complete repeat resection improved survival. Moreover, the use of intraoperative imaging adjuncts can maximise tumour resection, whilst minimising the risk of neurological deficit.
Keywords: Glioblastoma; Recurrent; Repeat; Surgical resection.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
