

Effects of prone positioning on lung mechanical power components in patients with acute respiratory distress syndrome: a physiologic study
- PMID: 38491457
- PMCID: PMC10941550
- DOI: 10.1186/s13054-024-04867-6
Effects of prone positioning on lung mechanical power components in patients with acute respiratory distress syndrome: a physiologic study
Abstract
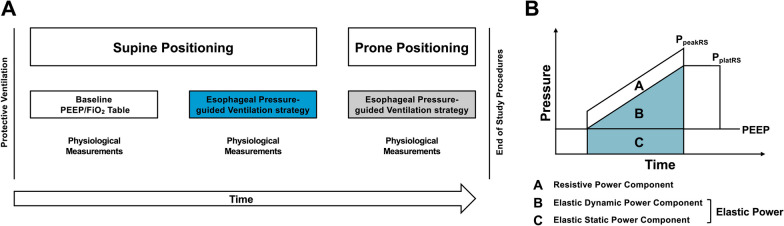
Background: Prone positioning (PP) homogenizes ventilation distribution and may limit ventilator-induced lung injury (VILI) in patients with moderate to severe acute respiratory distress syndrome (ARDS). The static and dynamic components of ventilation that may cause VILI have been aggregated in mechanical power, considered a unifying driver of VILI. PP may affect mechanical power components differently due to changes in respiratory mechanics; however, the effects of PP on lung mechanical power components are unclear. This study aimed to compare the following parameters during supine positioning (SP) and PP: lung total elastic power and its components (elastic static power and elastic dynamic power) and these variables normalized to end-expiratory lung volume (EELV).
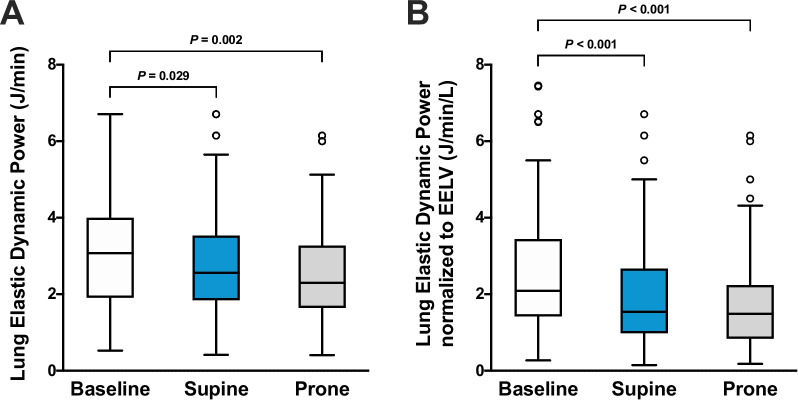
Methods: This prospective physiologic study included 55 patients with moderate to severe ARDS. Lung total elastic power and its static and dynamic components were compared during SP and PP using an esophageal pressure-guided ventilation strategy. In SP, the esophageal pressure-guided ventilation strategy was further compared with an oxygenation-guided ventilation strategy defined as baseline SP. The primary endpoint was the effect of PP on lung total elastic power non-normalized and normalized to EELV. Secondary endpoints were the effects of PP and ventilation strategies on lung elastic static and dynamic power components non-normalized and normalized to EELV, respiratory mechanics, gas exchange, and hemodynamic parameters.
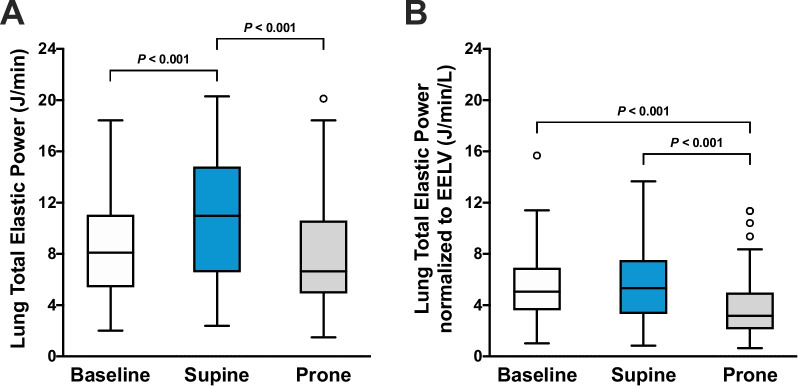
Results: Lung total elastic power (median [interquartile range]) was lower during PP compared with SP (6.7 [4.9-10.6] versus 11.0 [6.6-14.8] J/min; P < 0.001) non-normalized and normalized to EELV (3.2 [2.1-5.0] versus 5.3 [3.3-7.5] J/min/L; P < 0.001). Comparing PP with SP, transpulmonary pressures and EELV did not significantly differ despite lower positive end-expiratory pressure and plateau airway pressure, thereby reducing non-normalized and normalized lung elastic static power in PP. PP improved gas exchange, cardiac output, and increased oxygen delivery compared with SP.
Conclusions: In patients with moderate to severe ARDS, PP reduced lung total elastic and elastic static power compared with SP regardless of EELV normalization because comparable transpulmonary pressures and EELV were achieved at lower airway pressures. This resulted in improved gas exchange, hemodynamics, and oxygen delivery.
Trial registration: German Clinical Trials Register (DRKS00017449). Registered June 27, 2019. https://drks.de/search/en/trial/DRKS00017449.
Keywords: Acute respiratory distress syndrome; End-expiratory lung volume; Lung-protective ventilation; Mechanical power; Prone positioning; Respiratory mechanics; Ventilator-induced lung injury.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Positive end-expiratory pressure management in patients with severe ARDS: implications of prone positioning and extracorporeal membrane oxygenation.Crit Care. 2024 Aug 26;28(1):277. doi: 10.1186/s13054-024-05059-y. Crit Care. 2024. PMID: 39187853 Free PMC article. Review.
-
Effects of different positive end-expiratory pressure titration strategies during prone positioning in patients with acute respiratory distress syndrome: a prospective interventional study.Crit Care. 2022 Mar 26;26(1):82. doi: 10.1186/s13054-022-03956-8. Crit Care. 2022. PMID: 35346325 Free PMC article.
-
Effects of positive end-expiratory pressure strategy in supine and prone position on lung and chest wall mechanics in acute respiratory distress syndrome.Ann Intensive Care. 2018 Sep 10;8(1):86. doi: 10.1186/s13613-018-0434-2. Ann Intensive Care. 2018. PMID: 30203117 Free PMC article.
-
Effect of prone positioning on end-expiratory lung volume, strain and oxygenation change over time in COVID-19 acute respiratory distress syndrome: A prospective physiological study.Front Med (Lausanne). 2022 Dec 2;9:1056766. doi: 10.3389/fmed.2022.1056766. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36530873 Free PMC article.
-
Ventilator-induced lung injury during controlled ventilation in patients with acute respiratory distress syndrome: less is probably better.Expert Rev Respir Med. 2018 May;12(5):403-414. doi: 10.1080/17476348.2018.1457954. Epub 2018 Mar 29. Expert Rev Respir Med. 2018. PMID: 29575957 Review.
Cited by
-
[Prone positioning for acute respiratory distress syndrome in adults : Update on the physiological effects, indications and implementation].Anaesthesiologie. 2024 Aug;73(8):556-568. doi: 10.1007/s00101-024-01439-9. Anaesthesiologie. 2024. PMID: 39080082 Review. German.
-
Positive end-expiratory pressure management in patients with severe ARDS: implications of prone positioning and extracorporeal membrane oxygenation.Crit Care. 2024 Aug 26;28(1):277. doi: 10.1186/s13054-024-05059-y. Crit Care. 2024. PMID: 39187853 Free PMC article. Review.
-
The effects of prolonged prone positioning on response and prognosis in patients with acute respiratory distress syndrome: a retrospective cohort study.J Intensive Care. 2025 May 7;13(1):24. doi: 10.1186/s40560-025-00795-x. J Intensive Care. 2025. PMID: 40336057 Free PMC article.
-
The Mechanical Power in Patients with Acute Respiratory Distress Syndrome Undergoing Prone Positioning Can Predict Mortality.Diagnostics (Basel). 2025 Jan 12;15(2):158. doi: 10.3390/diagnostics15020158. Diagnostics (Basel). 2025. PMID: 39857042 Free PMC article.
-
Assessment of recruitment from CT to the bedside: challenges and future directions.Crit Care. 2025 Feb 6;29(1):64. doi: 10.1186/s13054-025-05263-4. Crit Care. 2025. PMID: 39915886 Free PMC article. Review.
References
-
- Cornejo RA, Diaz JC, Tobar EA, Bruhn AR, Ramos CA, Gonzalez RA, Repetto CA, Romero CM, Galvez LR, Llanos O, et al. Effects of prone positioning on lung protection in patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2013;188(4):440–448. doi: 10.1164/rccm.201207-1279OC. - DOI - PubMed
-
- Sarge T, Baedorf-Kassis E, Banner-Goodspeed V, Novack V, Loring SH, Gong MN, Cook D, Talmor D, Beitler JR. EPVent-2 study group: effect of esophageal pressure-guided positive end-expiratory pressure on survival from acute respiratory distress syndrome: a risk-based and mechanistic reanalysis of the EPVent-2 trial. Am J Respir Crit Care Med. 2021;204(10):1153–1163. doi: 10.1164/rccm.202009-3539OC. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
