

Obesity: the perfect storm for heart failure
- PMID: 38491741
- PMCID: PMC11287355
- DOI: 10.1002/ehf2.14641
Obesity: the perfect storm for heart failure
Abstract
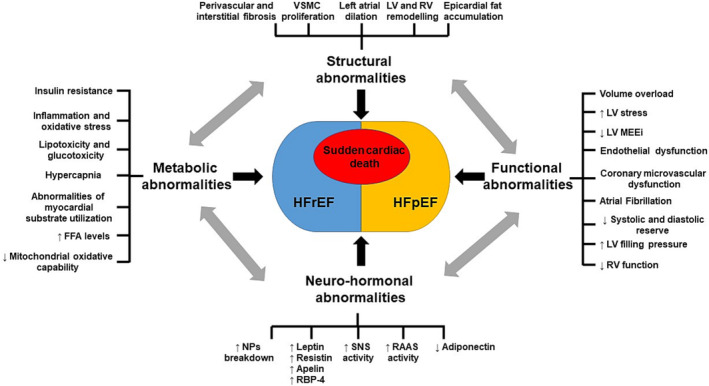
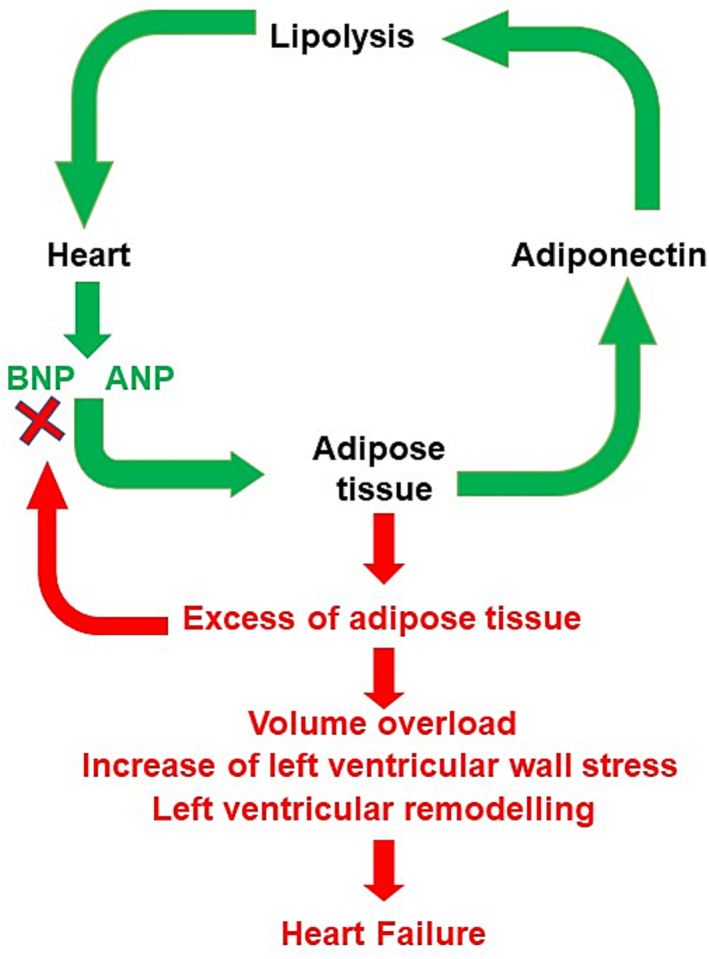
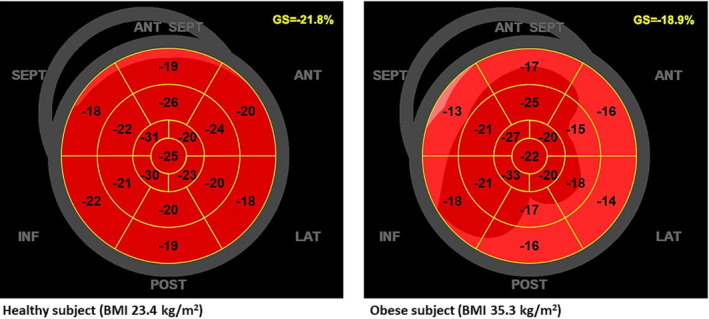
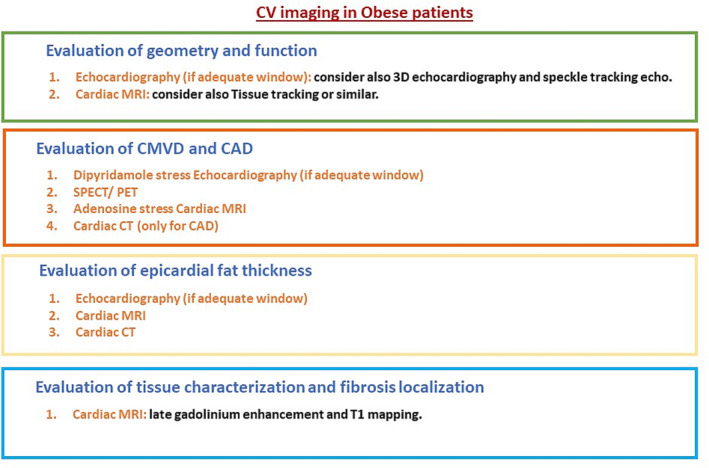
Obesity condition causes morphological and functional alterations involving the cardiovascular system. These can represent the substrates for different cardiovascular diseases, such as atrial fibrillation, coronary artery disease, sudden cardiac death, and heart failure (HF) with both preserved ejection fraction (EF) and reduced EF. Different pathogenetic mechanisms may help to explain the association between obesity and HF including left ventricular remodelling and epicardial fat accumulation, endothelial dysfunction, and coronary microvascular dysfunction. Multi-imaging modalities are required for appropriate recognition of subclinical systolic dysfunction typically associated with obesity, with echocardiography being the most cost-effective technique. Therapeutic approach in patients with obesity and HF is challenging, particularly regarding patients with preserved EF in which few strategies with high level of evidence are available. Weight loss is of extreme importance in patients with obesity and HF, being a primary therapeutic intervention. Sodium-glucose co-transporter-2 inhibitors have been recently introduced as a novel tool in the management of HF patients. The present review aims at analysing the most recent studies supporting pathogenesis, diagnosis, and management in patients with obesity and HF.
Keywords: Atrial fibrillation; Direct‐acting oral anticoagulants; Heart failure; Implantable cardioverter–defibrillators; Left ventricular remodelling; Natriuretic peptides; Obesity; Sacubitril/valsartan; Sodium–glucose co‐transporter‐2 inhibitors; Sudden cardiac death.
© 2024 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
-
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Bohm M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2021;42:3599‐3726. doi:10.1093/eurheartj/ehab368 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
