

Peroneal artery injury potential due to different syndesmosis screw placement options: a simulation study with lower extremity computed tomography angiography
- PMID: 38492060
- PMCID: PMC11093777
- DOI: 10.1007/s00402-024-05258-w
Peroneal artery injury potential due to different syndesmosis screw placement options: a simulation study with lower extremity computed tomography angiography
Abstract
Introduction: The aim of this study is to assess the risk of peroneal artery injury of hardware placement at the fixation of syndesmotic injuries.
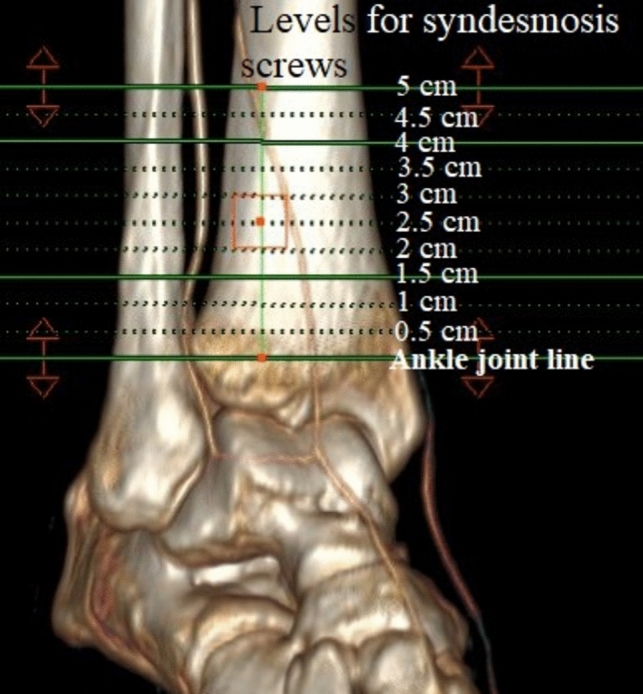
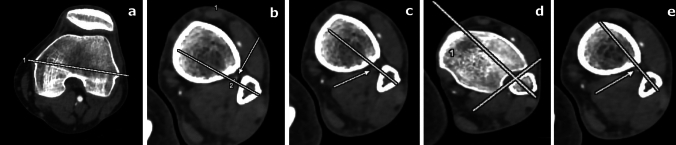
Materials and methods: The lower extremity computed tomography angiography was used to design the study. The syndesmosis screw placement range was simulated every 0.5 cm, from 0.5 to 5 cm proximal to the ankle joint. The screw axes were drawn as 20°, 30° or individual angle according to the femoral epicondylar axis. The proximity between the screw axis and the peroneal artery was measured in millimeters. Potential peroneal artery injury was noted if the distance between the peroneal artery to the axis of the simulated screw was within the outer shaft radius of the simulated screw. The Pearson chi-square test was used and a p-value < 0.05 was considered significant.
Results: The potential for injury to the peroneal artery increased as the syndesmosis screw level rose proximally from the ankle joint level or as the diameter of the syndesmosis screw increasds. In terms of syndesmosis screw trajection, the lowest risk of injury was observed with the syndesmosis screw angle of 20°. Simulations with a screw diameter of 3.5 mm exhibited the least potential for peroneal artery injury.
Conclusion: Thanks to this radiological anatomy simulation study, we believe that we have increased the awareness of the peroneal artery potential in syndesmosis screw application. Each syndesmosis screw placement option may have different potential for injury to the peroneal artery. To decrease the peroneal artery injury potential, we recommend the followings. If individual syndesmosis screw angle trajection can be measured, place the screw 1.5 cm proximal to the ankle joint using a 3.5 mm screw shaft. If not, fix it with 30° trajection regardless of the screw diameter at the same level. If the most important issue is the peroneal artery circulation, use the screw level up to 1 cm proximal to the ankle joint regardless of the screw angle trajection and screw diameter.
Keywords: Computed tomography angiography; Iatrogenic injury; Peroneal artery; Syndesmosis screw.
© 2024. The Author(s).
Figures
Similar articles
-
Ankle syndesmotic fixation using two screws: risk of injury to the perforating branch of the peroneal artery.J Foot Ankle Surg. 2014 Sep-Oct;53(5):534-8. doi: 10.1053/j.jfas.2014.04.006. Epub 2014 May 27. J Foot Ankle Surg. 2014. PMID: 24875967
-
A prospective randomised study comparing TightRope and syndesmotic screw fixation for accuracy and maintenance of syndesmotic reduction assessed with bilateral computed tomography.Injury. 2015;46(6):1119-26. doi: 10.1016/j.injury.2015.02.004. Epub 2015 Feb 21. Injury. 2015. PMID: 25769201 Clinical Trial.
-
Fixation of ankle syndesmotic injuries: comparison of tightrope fixation and syndesmotic screw fixation for accuracy of syndesmotic reduction.Am J Sports Med. 2012 Dec;40(12):2828-35. doi: 10.1177/0363546512461480. Epub 2012 Oct 10. Am J Sports Med. 2012. PMID: 23051785
-
Comparison of suture button fixation and syndesmotic screw fixation in the treatment of distal tibiofibular syndesmosis injury: A systematic review and meta-analysis.Int J Surg. 2018 Dec;60:120-131. doi: 10.1016/j.ijsu.2018.11.007. Epub 2018 Nov 12. Int J Surg. 2018. PMID: 30439535
-
Evaluation and management of injuries of the tibiofibular syndesmosis.Br Med Bull. 2014 Sep;111(1):101-15. doi: 10.1093/bmb/ldu020. Br Med Bull. 2014. PMID: 25190761 Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
