

Platinum chemotherapy for early triple-negative breast cancer
- PMID: 38492276
- PMCID: PMC10959715
- DOI: 10.1016/j.breast.2024.103712
Platinum chemotherapy for early triple-negative breast cancer
Abstract
Background: Triple-negative breast cancer (TNBC) is an aggressive subtype of breast cancer associated with shorter survival and a higher likelihood of recurrence. In early TNBC, platinum chemotherapy has been shown to improve pathological complete response (pCR); however, its effect on long-term survival outcomes has not been fully elucidated.
Methods: Randomised controlled trials examining neoadjuvant or adjuvant platinum chemotherapy for early TNBC were included. Primary outcomes were disease-free survival (DFS) and overall survival (OS). Secondary outcomes were pCR, treatment adherence, grade III or IV toxicity related to chemotherapy, and quality of life.
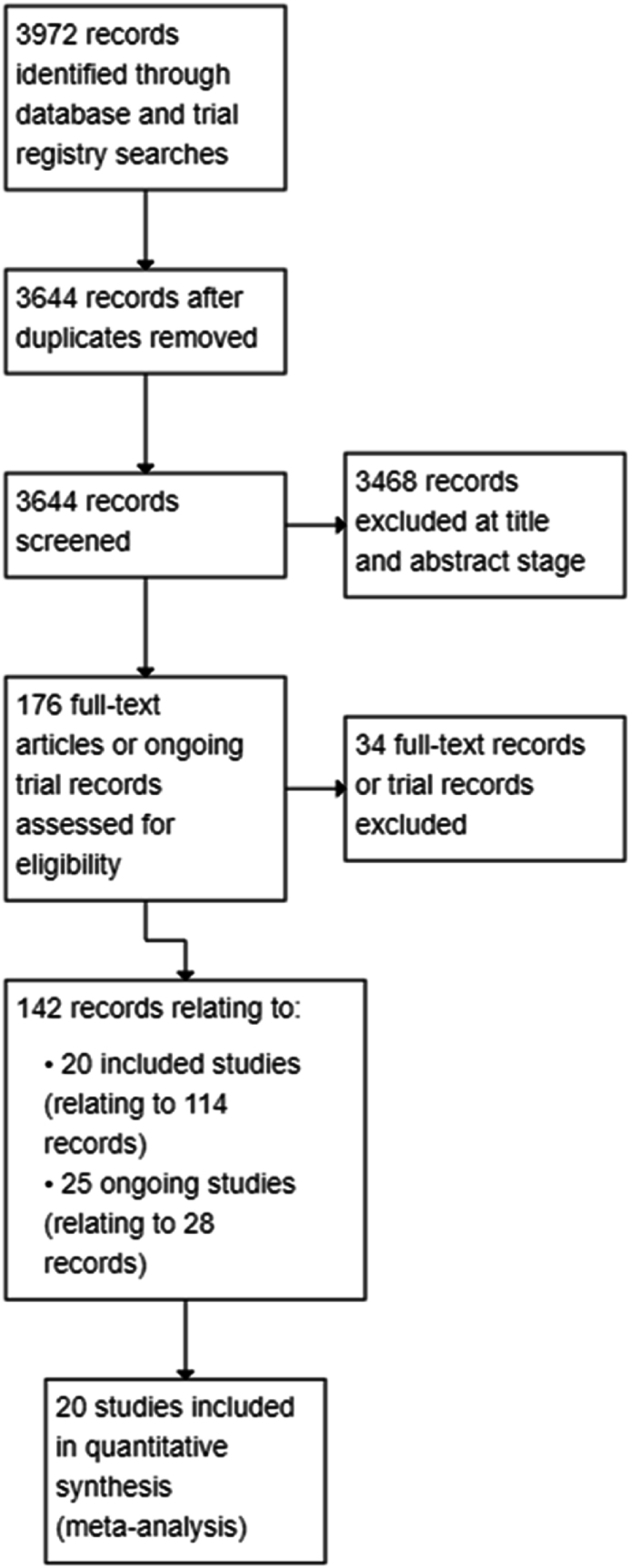
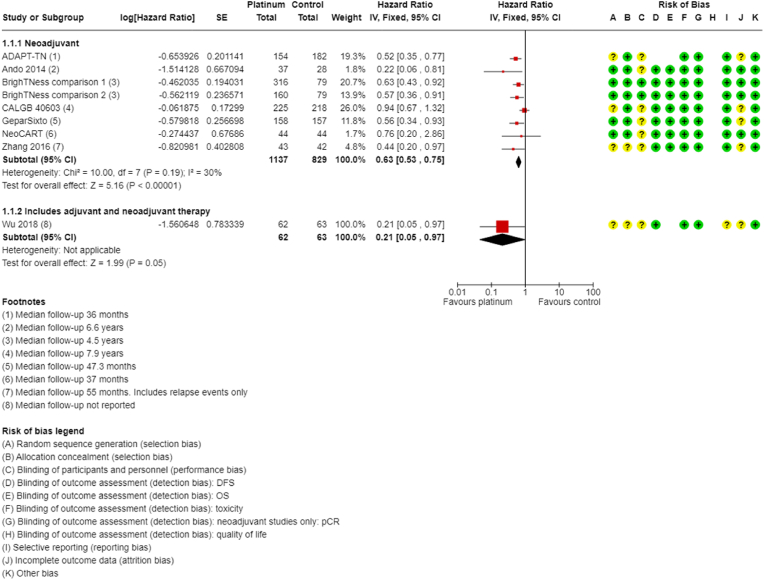
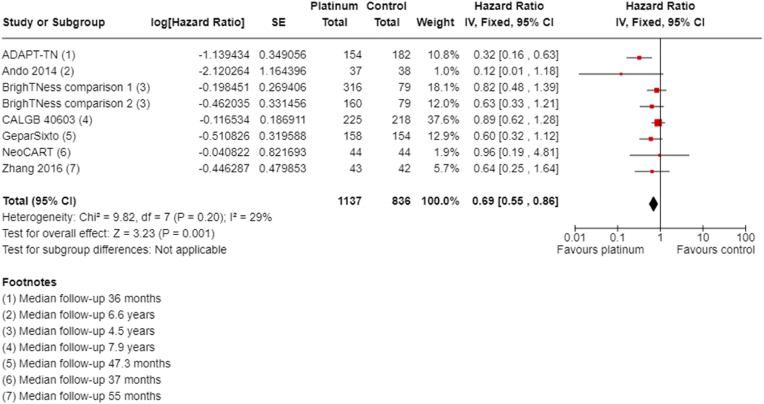
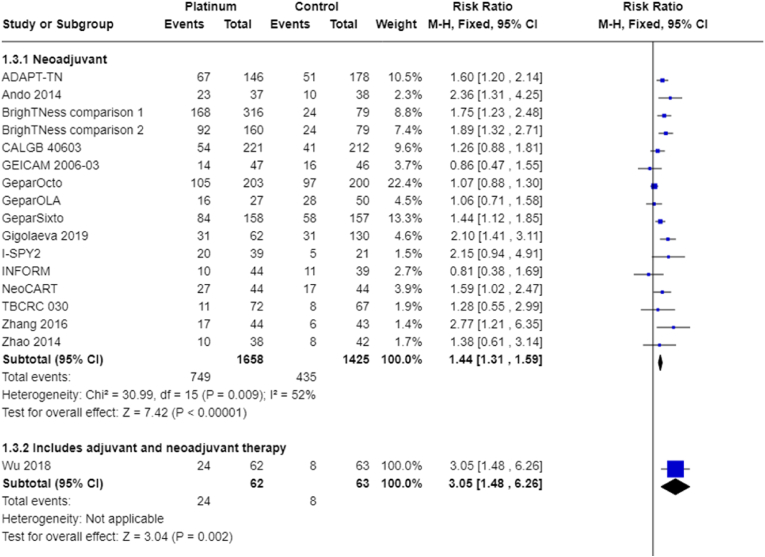
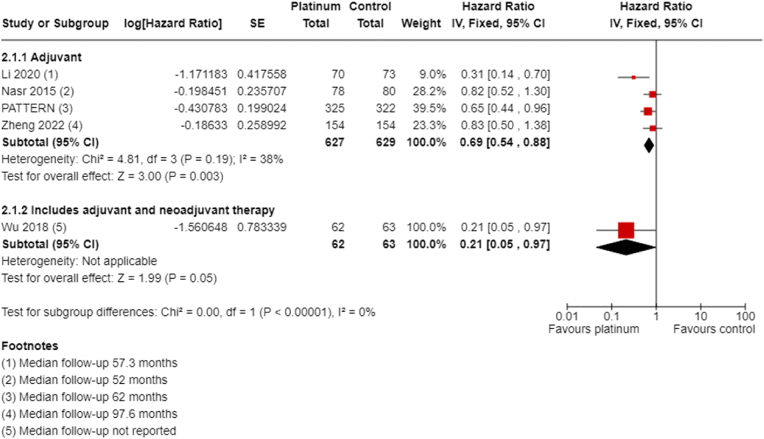
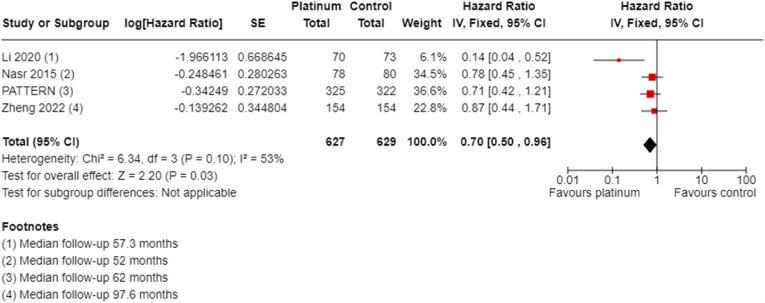
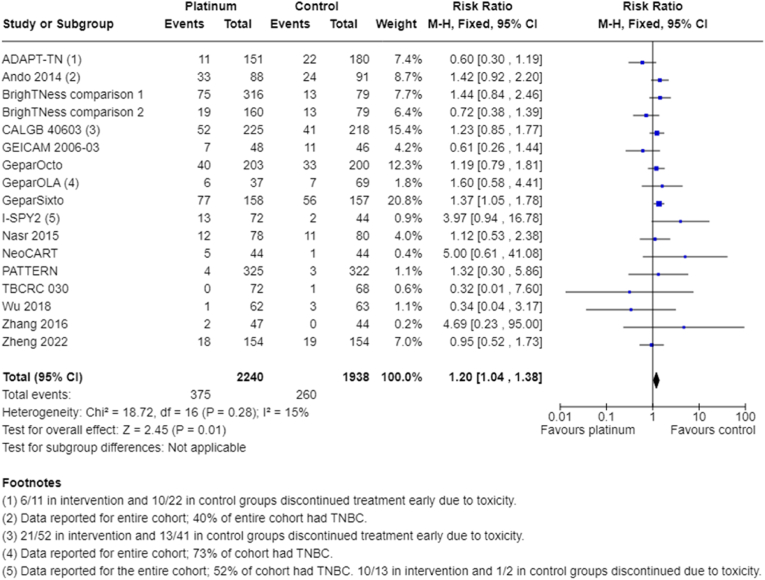
Results: From 3972 records, we included 20 published studies. All studies reporting DFS and OS used carboplatin. Inclusion of platinum chemotherapy improved DFS (neoadjuvant: hazard ratio (HR) 0.63, 95% confidence interval (CI) 0.53 to 0.75; adjuvant: HR 0.69, 95% CI 0.54 to 0.88) and OS (neoadjuvant: HR 0.69, 95% CI 0.55 to 0.86; adjuvant: 0.70, 95% CI 0.50 to 0.96). Our analysis confirmed platinum chemotherapy increased pCR rates (risk ratio (RR) 1.44, 95% CI 1.31 to 1.59). There were no differences seen in examined subgroups. Platinum chemotherapy was associated with reduced dose intensity and increased haematological toxicity.
Conclusions: Platinum-based chemotherapy using carboplatin in the adjuvant or neoadjuvant setting improves long-term outcomes of DFS and OS in early TNBC, with no evidence of differences by subgroup. This was at the cost of more frequent chemotherapy delays and dose reductions, and greater haematological toxicity. These findings support the use of platinum-based chemotherapy for people with early TNBC.
Keywords: Carboplatin; Platinum; Triple-negative breast cancer.
Copyright © 2024 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Ferlay J, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, et al, editor(s). Cancer today (powered by GLOBOCAN 2018) IARC CancerBase No. 15. publications.iarc.fr/Databases/Iarc-Cancerbases/Cancer-Today-Powered-By-... (accessed 17 July 2020).
-
- Foulkes W.D., Smith I.E., Reis-Filho J.S. Triple-negative breast cancer. N Engl J Med. 2010;363(20):1938–1948. - PubMed
-
- Cortazar P., Zhang L., Untch M., Mehta K., Costantino J.P., Wolmark N., et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384(9938):164–172. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
