

Risk of COVID-19 Hospitalization and Protection Associated With mRNA Vaccination Among US Adults With Psychiatric Disorders
- PMID: 38494192
- PMCID: PMC10944689
- DOI: 10.1111/irv.13269
Risk of COVID-19 Hospitalization and Protection Associated With mRNA Vaccination Among US Adults With Psychiatric Disorders
Abstract
Background: Although psychiatric disorders have been associated with reduced immune responses to other vaccines, it remains unknown whether they influence COVID-19 vaccine effectiveness (VE). This study evaluated risk of COVID-19 hospitalization and estimated mRNA VE stratified by psychiatric disorder status.
Methods: In a retrospective cohort analysis of the VISION Network in four US states, the rate of laboratory-confirmed COVID-19-associated hospitalization between December 2021 and August 2022 was compared across psychiatric diagnoses and by monovalent mRNA COVID-19 vaccination status using Cox proportional hazards regression.
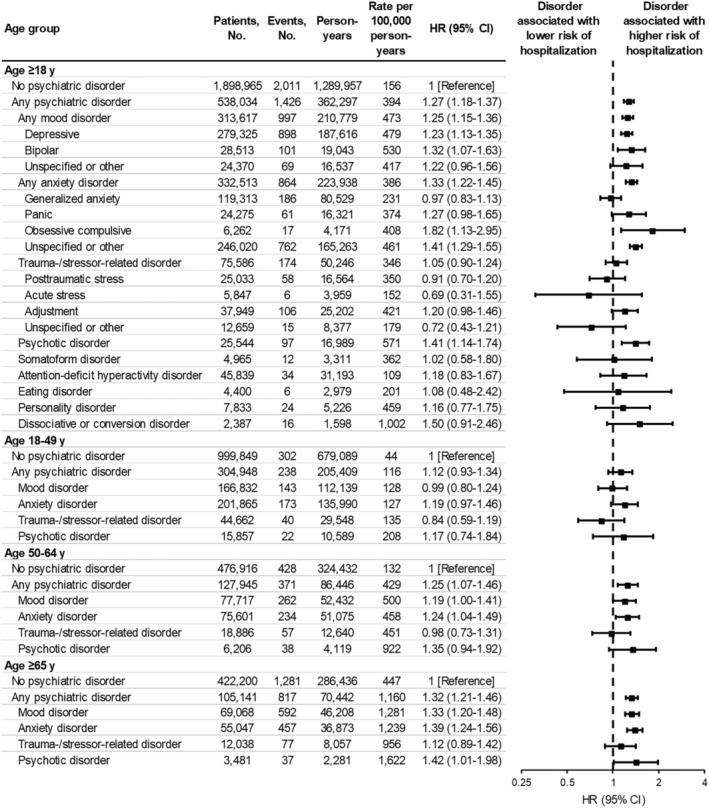
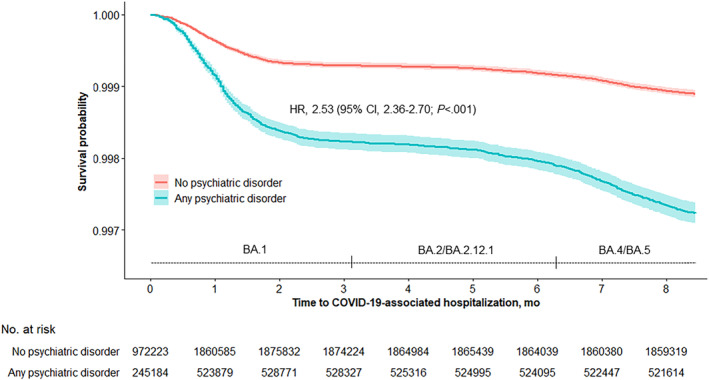
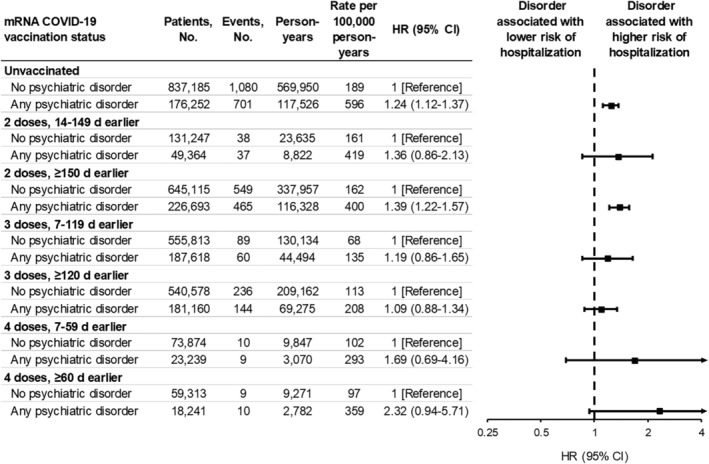
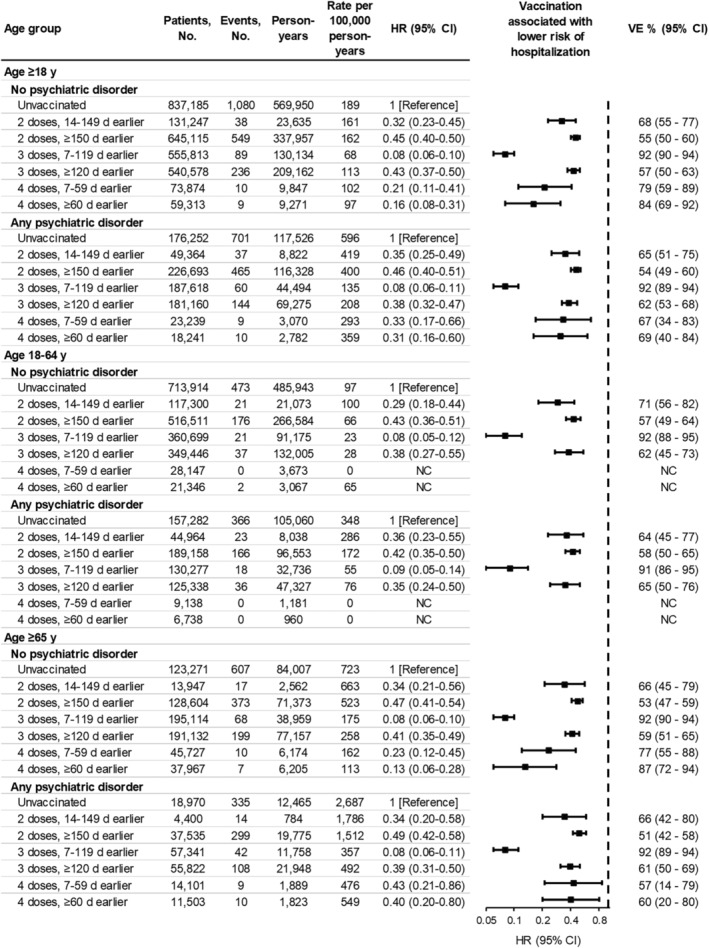
Results: Among 2,436,999 adults, 22.1% had ≥1 psychiatric disorder. The incidence of COVID-19-associated hospitalization was higher among patients with any versus no psychiatric disorder (394 vs. 156 per 100,000 person-years, p < 0.001). Any psychiatric disorder (adjusted hazard ratio [aHR], 1.27; 95% CI, 1.18-1.37) and mood (aHR, 1.25; 95% CI, 1.15-1.36), anxiety (aHR, 1.33, 95% CI, 1.22-1.45), and psychotic (aHR, 1.41; 95% CI, 1.14-1.74) disorders were each significant independent predictors of hospitalization. Among patients with any psychiatric disorder, aHRs for the association between vaccination and hospitalization were 0.35 (95% CI, 0.25-0.49) after a recent second dose, 0.08 (95% CI, 0.06-0.11) after a recent third dose, and 0.33 (95% CI, 0.17-0.66) after a recent fourth dose, compared to unvaccinated patients. Corresponding VE estimates were 65%, 92%, and 67%, respectively, and were similar among patients with no psychiatric disorder (68%, 92%, and 79%).
Conclusion: Psychiatric disorders were associated with increased risk of COVID-19-associated hospitalization. However, mRNA vaccination provided similar protection regardless of psychiatric disorder status, highlighting its benefit for individuals with psychiatric disorders.
Keywords: COVID-19; anxiety disorders; electronic health records; epidemiology; mental disorders; mood disorders; psychotic disorders; vaccination.
© 2024 The Authors. Influenza and Other Respiratory Viruses published by John Wiley & Sons Ltd.
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. During the conduct of the study, all Westat‐ and Kaiser Permanente Northern California Division of Research‐affiliated authors reported receiving contractual support from the CDC via payments made to their respective institutions. Additionally, all authors affiliated with Baylor Scott & White Health, Children's Minnesota, Columbia University Irving Medical Center, HealthPartners Institute, Intermountain Healthcare, Kaiser Permanente Center for Health Research, Regenstrief Institute, University of Colorado Anschutz Medical Campus, and Vanderbilt University Medical Center reported receiving contractual support from the CDC during the conduct of the study, via subcontracts from Westat, Inc. with payments made to their respective institutions. Unrelated to the submitted work, the following disclosures were reported from the past 36 months: Dr. Gaglani received grants directly from CDC and from CDC via subcontracts from Abt Associates and Vanderbilt University Medical Center to her institution; Dr. Naleway received grants from Pfizer and Vir Biotechnology; Dr. Klein received grants from Pfizer, Merck, GlaxoSmithKline, and Sanofi Pasteur; Dr. Dixon reported receiving grants from CDC, NIH, AHRQ, and the U.S. Department of Veterans Affairs to his institution as well as personal fees from Elsevier and Springer Nature and consulting fees from Merck and Co.; Dr. Rao received grants from GSK; and Dr. Murthy received grants from CDC to his institution. The other authors declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
