

Systemic and Tumor-directed Therapy for Oligorecurrent Metastatic Prostate Cancer (SATURN): Primary Endpoint Results from a Phase 2 Clinical Trial
- PMID: 38494380
- PMCID: PMC11386258
- DOI: 10.1016/j.eururo.2024.01.021
Systemic and Tumor-directed Therapy for Oligorecurrent Metastatic Prostate Cancer (SATURN): Primary Endpoint Results from a Phase 2 Clinical Trial
Abstract
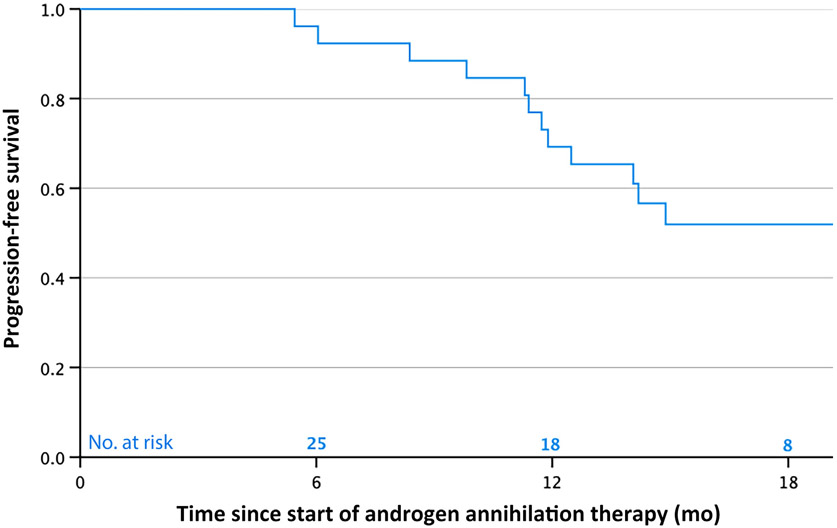
Nearly all men with metastatic hormone-sensitive prostate cancer treated with intermittent androgen deprivation therapy (ADT) experience recurrence within 6 mo of testosterone recovery. We conducted a single-arm phase 2 trial to evaluate whether addition of dual androgen receptor pathway inhibitors (ARPIs) and metastasis-directed stereotactic body radiotherapy (SBRT) to intermittent ADT improves recurrence rates for men with between one and five nonvisceral, extrapelvic metastases on prostate-specific membrane antigen positron emission tomography/computed tomography after prior radical prostatectomy. Patients received 6 mo of androgen annihilation therapy (AAT; leuprolide, abiraterone acetate plus prednisone, and apalutamide) and metastasis-directed SBRT. The primary endpoint was the percentage of patients with prostate-specific antigen (PSA) <0.05 ng/ml 6 mo after testosterone recovery (≥150 ng/dl), with the study powered to detect an improvement from 1% to 12%. We enrolled 28 men between March 2021 and June 2022. Median follow-up was 20 mo (interquartile range 16-22). Twenty-six patients (93%) completed SBRT with 6 mo of hormone therapy, of whom six discontinued at least one ARPI; two patients withdrew prematurely. At 6 mo after testosterone recovery, PSA was maintained at <0.05 ng/ml in 13/26 patients (50%, 95% confidence interval 32-67%). Rates of grade 2 and 3 AAT toxicity were 21% and 21%. The results confirm that addition of metastasis-directed SBRT to highly potent systemic therapy can maintain low PSA after testosterone recovery, although further studies are needed to clarify the optimal systemic therapy regimen. PATIENT SUMMARY: We tested a combination of intensified hormone therapy (called androgen annihilation therapy) and radiotherapy targeted at metastases in men with recurrence of metastatic prostate cancer. We found that half of patients were recurrence-free 6 months after their testosterone level recovered, and that less than a quarter of patients experienced a severe drug-related side effect. Overall, this appears to be an effective therapy with acceptable side effects. This trial is registered on ClinicalTrials.gov as NCT03902951.
Keywords: Abiraterone acetate; Androgen annihilation therapy; Apalutamide; Leuprolide; Metastasis-directed therapy; Oligorecurrence; Prostate cancer; Stereotactic body radiotherapy.
Copyright © 2024 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
