

Single center experience with ALPPS and timing with stage 2 in patients with fibrotic/cirrhotic liver
- PMID: 38494567
- PMCID: PMC11341627
- DOI: 10.1007/s13304-024-01782-x
Single center experience with ALPPS and timing with stage 2 in patients with fibrotic/cirrhotic liver
Abstract
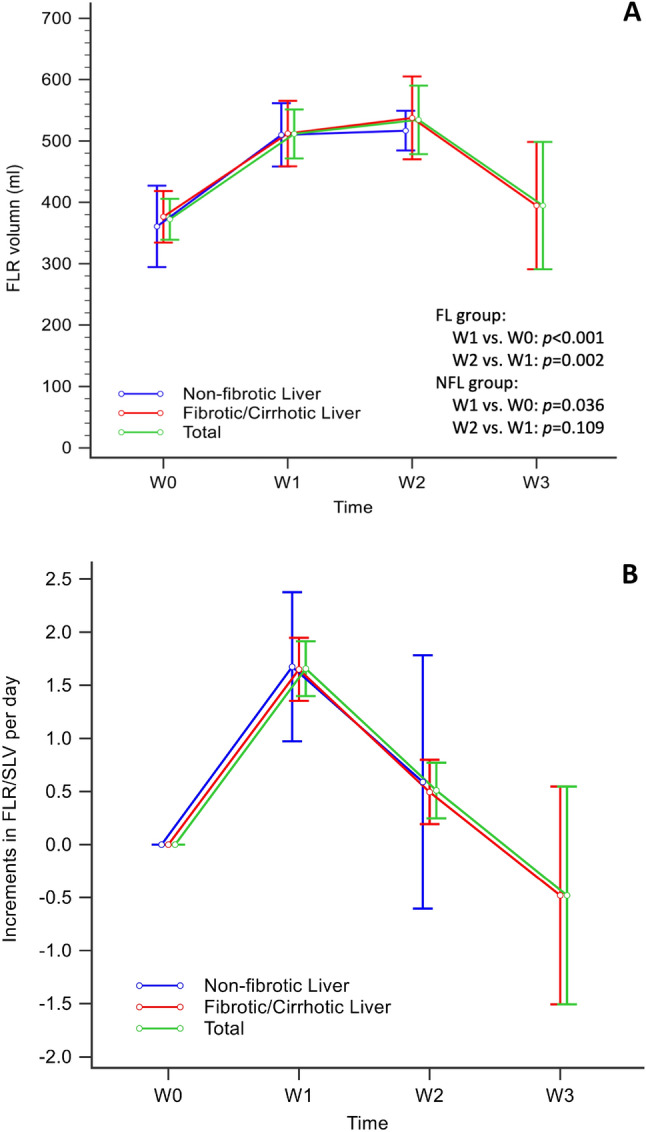
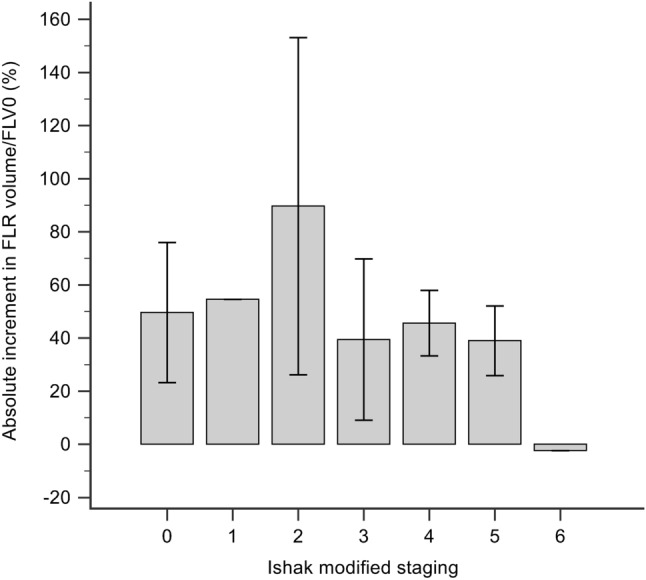
Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) is a novel procedure for major resection in patients with insufficient future liver remnant (FLR). Effective FLR augmentation is pivotal in the completion of ALPPS. Liver fibrosis/cirrhosis associated with chronic viral hepatitis impairs liver regeneration. To investigate the augmentation of FLR in associating ALPPS between patients with fibrotic/cirrhotic livers (FL) and non-fibrotic livers (NFL) and compare their short-term clinical outcomes and long-term survival. Patients were divided into two groups based on the Ishak modified staging: non-fibrotic liver group (NFL, stage 0) and fibrotic/cirrhotic liver group (FL, stage 1-5/6). Weekly liver regeneration in FLR, perioperative data, and survival outcomes were investigated. Twenty-seven patients with liver tumors underwent ALPPS (NFL, n = 7; FL, n = 20). NFL and FL patients had viral hepatitis (28.6% [n = 2] and 95% [n = 19]), absolute FLR volume increments of 134.90 ml and 161.85 ml (p = 0.825), and rates of hypertrophy were 16.46 ml/day and 13.66 ml/day (p = 0.507), respectively. In the FL group, baseline FLR volume was 360.13 ml, postoperatively it increased to a plateau (542.30 ml) in week 2 and declined (378.45 ml) in week 3. One patient (3.7%) with cirrhotic liver (stage 6) failed to proceed to ALPPS-II. The overall ALPPS-related major complication rate was 7.4%. ALPPS is feasible for fibrotic liver patients classified by Ishak modified stages ≤ 5. After ALPPS-I, 14 days for FLR augmentation seems an appropriate waiting time to reach a maximum FLR volume in these patients.
Keywords: ALPPS; Hepatocellular carcinoma; Liver fibrosis/cirrhosis; Liver regeneration; Remnant liver volume; Viral hepatitis.
© 2024. The Author(s).
Conflict of interest statement
The authors declare they have no conflicts of interest.
Figures


References
-
- Schnitzbauer AA, Lang SA, Goessmann H, Nadalin S, Baumgart J, Farkas SA et al (2012) Right portal vein ligation combined with in situ splitting induces rapid left lateral liver lobe hypertrophy enabling 2-staged extended right hepatic resection in small-for-size settings. Ann Surg 255(3):405–414. 10.1097/SLA.0b013e31824856f5 10.1097/SLA.0b013e31824856f5 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
