

Proportion of Antipsychotics with CYP2D6 Pharmacogenetic (PGx) Associations Prescribed in an Early Intervention in Psychosis (EIP) Cohort: A Cross-Sectional Study
- PMID: 38494658
- PMCID: PMC11010551
- DOI: 10.1177/02698811241238283
Proportion of Antipsychotics with CYP2D6 Pharmacogenetic (PGx) Associations Prescribed in an Early Intervention in Psychosis (EIP) Cohort: A Cross-Sectional Study
Abstract
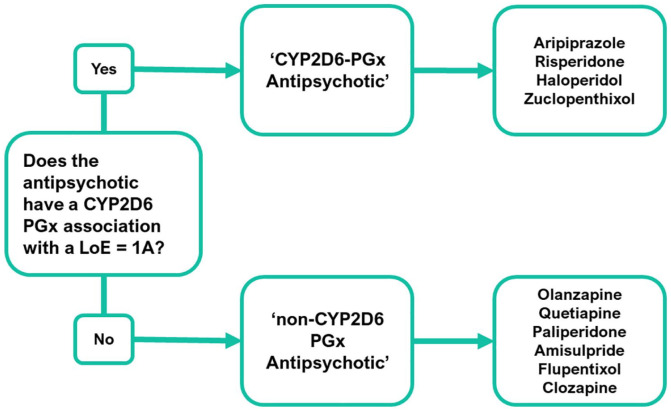
Background: Prescribing drugs for psychosis (antipsychotics) is challenging due to high rates of poor treatment outcomes, which are in part explained by an individual's genetics. Pharmacogenomic (PGx) testing can help clinicians tailor the choice or dose of psychosis drugs to an individual's genetics, particularly psychosis drugs with known variable response due to CYP2D6 gene variants ('CYP2D6-PGx antipsychotics').
Aims: This study aims to investigate differences between demographic groups prescribed 'CYP2D6-PGx antipsychotics' and estimate the proportion of patients eligible for PGx testing based on current pharmacogenomics guidance.
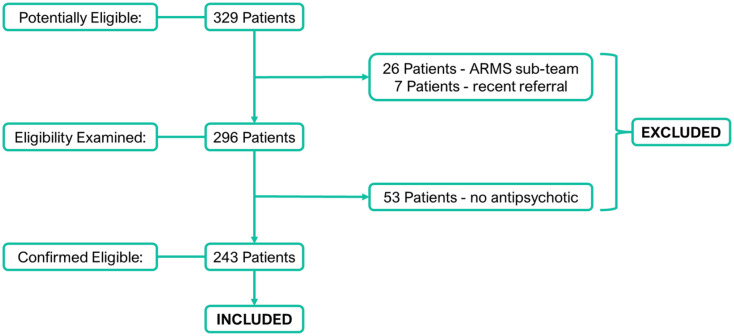
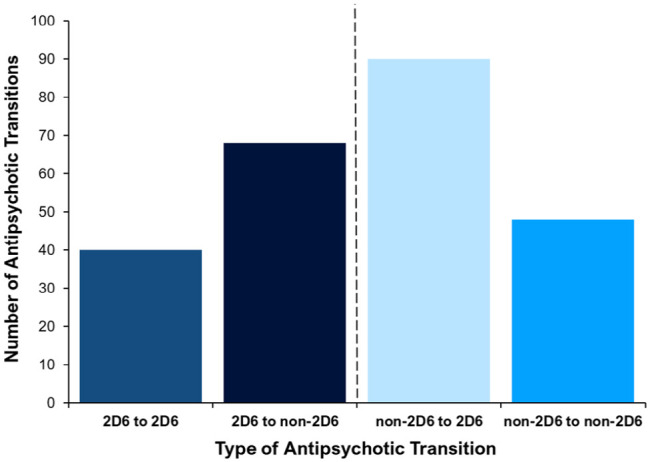
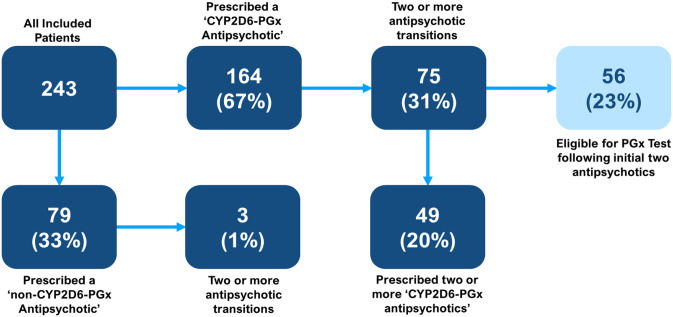
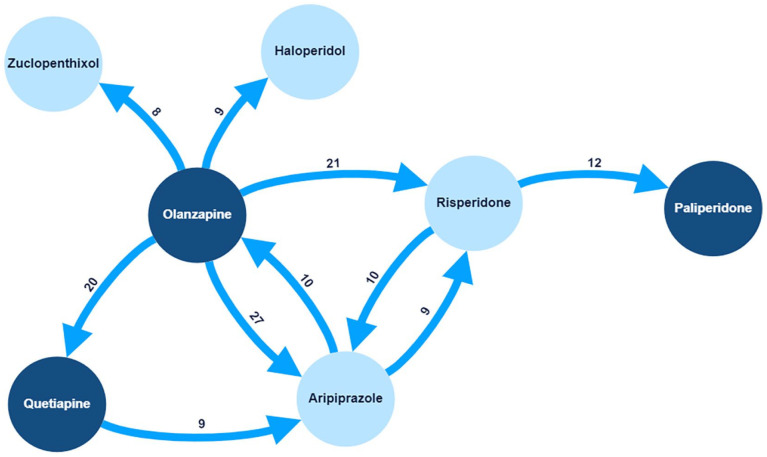
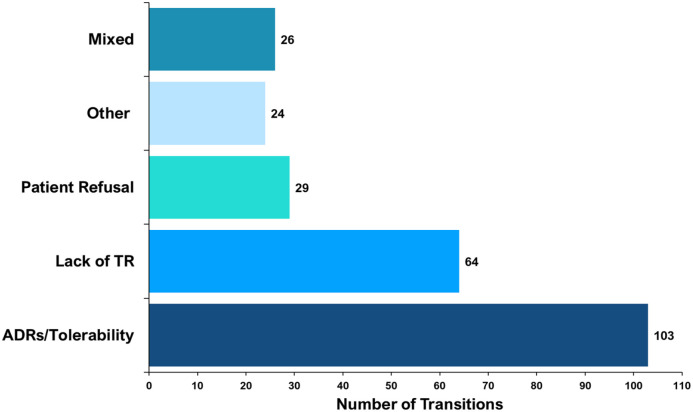
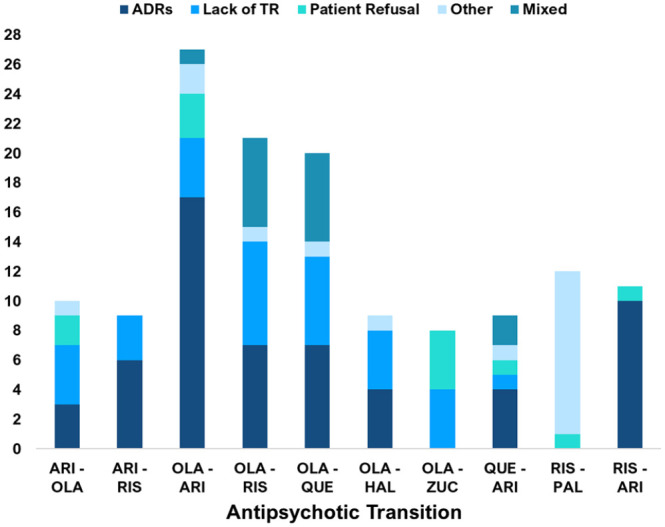
Methods: A cross-sectional study took place extracting data from 243 patients' medical records to explore psychosis drug prescribing, including drug transitions. Demographic data such as age, sex, ethnicity, and clinical sub-team were collected and summarised. Descriptive statistics explored the proportion of 'CYP2D6-PGx antipsychotic' prescribing and the nature of transitions. We used logistic regression analysis to investigate associations between demographic variables and prescription of 'CYP2D6-PGx antipsychotic' versus 'non-CYP2D6-PGx antipsychotic'.
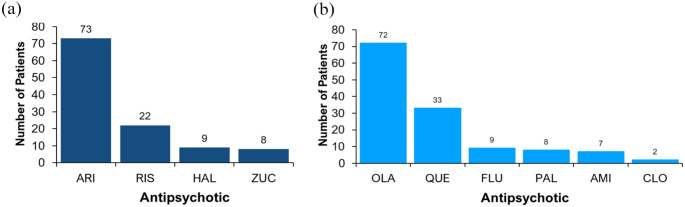
Results: Two-thirds (164) of patients had been prescribed a 'CYP2D6-PGx antipsychotic' (aripiprazole, risperidone, haloperidol or zuclopenthixol). Over a fifth (23%) of patients would have met the suggested criteria for PGx testing, following two psychosis drug trials. There were no statistically significant differences between age, sex, or ethnicity in the likelihood of being prescribed a 'CYP2D6-PGx antipsychotic'.
Conclusions: This study demonstrated high rates of prescribing 'CYP2D6-PGx-antipsychotics' in an EIP cohort, providing a rationale for further exploration of how PGx testing can be implemented in EIP services to personalise the prescribing of drugs for psychosis.
Keywords: Antipsychotics; Personalised Medicine; Pharmacogenetics; Pharmacogenomics; Psychosis; Receptor Antagonist (D2); Receptor Antagonist (D2, 5-HT2); Receptor Antagonist (D2, 5-HT2, NE, alpha-2); Receptor Partial Agonist (D2, 5-HT1A); Schizophrenia.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Update of
- doi: 10.2139/ssrn.4429212
References
-
- Alvarez-Jimenez M, Priede A, Hetrick SE, et al.. (2012) Risk factors for relapse following treatment for first episode psychosis: A systematic review and meta-analysis of longitudinal studies. Schizophrenia Res 139: 116–128. - PubMed
-
- Arranz MJ, Salazar J, Hernández MH. (2021) Pharmacogenetics of antipsychotics: Clinical utility and implementation. Behav Brain Res 401: 113058. - PubMed
-
- Barnes TR, Drake R, Paton C, et al.. (2020) Evidence-based guidelines for the pharmacological treatment of schizophrenia: Updated recommendations from the British Association for Psychopharmacology. J Psychopharmacol 34: 3–78. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
