

Effectiveness of a blended mobile-based lifestyle intervention in women with glucose intolerance after a recent history of gestational diabetes (MELINDA): a 1-year, prospective, multicentre, randomised controlled trial
- PMID: 38495521
- PMCID: PMC10940944
- DOI: 10.1016/j.eclinm.2024.102523
Effectiveness of a blended mobile-based lifestyle intervention in women with glucose intolerance after a recent history of gestational diabetes (MELINDA): a 1-year, prospective, multicentre, randomised controlled trial
Abstract
Background: Women with glucose intolerance after gestational diabetes mellitus (GDM) are at high risk to develop type 2 diabetes. Traditional lifestyle interventions in early postpartum have limited impact. We investigated the efficacy of a blended mobile-based lifestyle intervention in women with glucose intolerance after a recent history of GDM.
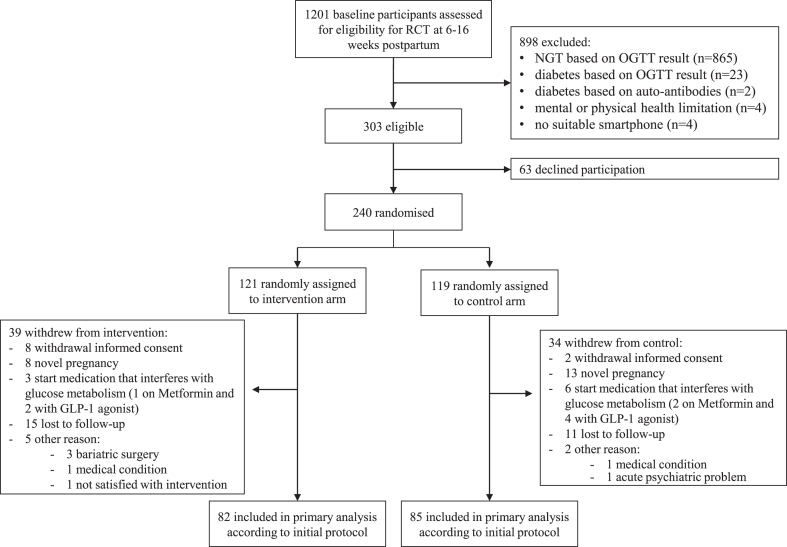
Methods: Prospective, double-arm, non-masked, multicentre randomised controlled trial (RCT) in which women with glucose intolerance, diagnosed 6-16 weeks after a GDM-complicated pregnancy, were assigned 1:1 to a one-year blended-care, telephone- and mobile-based lifestyle program (intervention) or usual care (control). Primary endpoint was the proportion of women able to achieve their weight goal (≥5% weight loss if prepregnancy BMI ≥ 25 kg/m2 or return to prepregnancy weight if prepregnancy BMI < 25 kg/m2) in the intention-to-treat sample. Key secondary outcomes were frequency of glucose intolerance, diabetes and metabolic syndrome, and lifestyle-related outcomes assessed with self-administered questionnaires. The study was registered in ClinicalTrials.gov (NCT03559621).
Findings: Between April 10th 2019 and May 13th 2022, 240 participants were assigned to the intervention (n = 121) or control group (n = 119), of which 167 (n = 82 in intervention and n = 85 in control group) completed the study. Primary outcome was achieved by 46.3% (56) of intervention participants compared to 43.3% (52) in the control group [odds ratio (OR) 1.13, 95% confidence interval (CI) 0.63-2.03, p = 0.680; risk ratio 1.07, 95% CI (0.78-1.48)]. Women in the intervention group developed significantly less often metabolic syndrome compared to the control group [7.3% (6) vs. 16.5% (14), OR 0.40, CI (0.22-0.72), p = 0.002], reported less sedentary behaviour and higher motivation for continuing healthy behaviours. In the intervention group, 84.1% (69) attended at least eight telephone sessions and 70.7% (58) used the app at least once weekly.
Interpretation: A blended, mobile-based lifestyle intervention was not effective in achieving weight goals, but reduced the risk to develop metabolic syndrome.
Funding: Research fund of University Hospitals Leuven, Novo Nordisk, Sanofi, AstraZeneca, Boehringer-Ingelheim, Lilly.
Keywords: Gestational diabetes mellitus; Lifestyle intervention; Mobile-based; Prediabetes; Prevention; Weight retention.
© 2024 The Author(s).
Conflict of interest statement
NM reports consulting fees from AstraZeneca and Boehringer Ingelheim, and serves on the speaker bureau for Novo Nordisk, AstraZeneca, Boehringer Ingelheim, Merck Sharp & Dohme. CBD reports consulting fees and honoraria for speaking for Abbott, AstraZeneca, Boehringer-Ingelheim, A. Menarini Diagnostics, Eli Lilly, Insulet, Medtronic, and Novo Nordisk. WV reports serving on the Merck Sharp & Dohme Advisory board on diabetes. LL has served on the speaker bureau for Novo Nordisk and Sanofi, and received support for attending a conference from Novo Nordisk. ChaM reports consulting fees from Novo Nordisk, Sanofi, Merck Sharp & Dohme, Eli Lilly, AstraZeneca, Boehringer Ingelheim, Roche, Medtronic, ActoBio Therapeutics, Pfizer, Insulet, and Zealand Pharma; and serves or has served on the speaker bureau for Novo Nordisk, Sanofi, Eli Lilly, Boehringer Ingelheim, AstraZeneca, and Novartis. Financial compensation for these activities has been received by KU Leuven. ChaM is president of EASD. All external support of EASD is to be found on www.easd.org. ChrM’s research is funded through internal KU Leuven funding, Fonds voor Wetenschappelijk Onderzoek (FWO), Vlaams Fonds voor Innovatie en Ondernemen (VLAIO), Horizon Europe and VLIR-UOS. He is chair of the KU Leuven Fund ‘Nutrition’, a donation-based fund to stimulate research on nutrition. He is a nonfunded member of the advisory board of Belgian Health and Nutrition Conference, non-funded board member of the Belgian Nutrition Society and the Flemish Society of Clinical Nutrition and Metabolism, non-funded associate editor of Frontiers in Nutrition and Scientific Reports. He is recipient of travel/accommodation expenses and small participation fee (<100€/meeting) as member of working groups of the Belgian Superior Health Council and Belgian Federal Agency of the Safety of the Food Chain. He is recipient of travel/accommodation expenses as member of the scientific advisory body of the Joint Programme Initiative Healthy Diet, Healthy Life, as co-chair ILSI Europe Task Force Dietary Intake and Exposure, as member ILSI Europe Task Force Nutrient Intake Optimisation. He is recipient of honoraria (<500€/year) as active member of the advisory board of NutriNews (Belgian Nutrition Information Centre). He is recipient of honoraria as jury-member of nutrition-related awards and reviewing EU-grants. He is recipient of royalties form a textbook (Handboek Voeding, ACCO). Honoraria are used to support research of PhD Students. KB reports research funding and receipt of study devices from Medtronic for the investigator-initiated CRISTAL study, receipt of study devices from Dexcom for the investigator-initiated GLORIA-study, receipt of study medication of Novo Nordisk for the investigator-initiated SERENA study, consulting fees from AstraZeneca and Lilly, and served on the speaker bureau for Novo Nordisk, AstraZeneca and Mundipharma. CaM received a doctoral grant for strategic basic research from Fonds Wetenschappelijk Onderzoek Flanders. KB received a fundamental clinical investigatorship from Fonds Wetenschappelijk Onderzoek Flanders (1800220 N). All disclosures are unrelated to the present work. All other authors declare no competing interests.
Figures
References
-
- American Diabetes Association Standards of medical care in diabetes-2021. Diabetes Care. 2021;44:S1–S232. - PubMed
-
- Buchanan T.A. Pancreatic B-cell defects in gestational diabetes: implications for the pathogenesis and prevention of type 2 diabetes. J Clin Endocrinol Metab. 2001;86:989–993. - PubMed
-
- Gerstein H.C., Santaguida P., Raina P., et al. Annual incidence and relative risk of diabetes in people with various categories of dysglycemia: a systematic overview and meta-analysis of prospective studies. Diabetes Res Clin Pract. 2007;78:305–312. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
