

Identification of immunological patterns characterizing immune-related psoriasis reactions in oncological patients in therapy with anti-PD-1 checkpoint inhibitors
- PMID: 38495872
- PMCID: PMC10940473
- DOI: 10.3389/fimmu.2024.1346687
Identification of immunological patterns characterizing immune-related psoriasis reactions in oncological patients in therapy with anti-PD-1 checkpoint inhibitors
Abstract
Introduction: Immunotherapy with biologics targeting programmed cell death protein-1 (PD-1) is highly effective in the treatment of various malignancies. Nevertheless, it is frequently responsible for unexpected cutaneous manifestations, including psoriasis-like dermatitis. The pathogenesis of anti-PD-1-induced psoriasis has yet to be clarified, even though it is plausible that some innate and adaptive immunity processes are in common with canonical psoriasis. The genetic predisposition to psoriasis of patients could also be a contributing factor. Here, we investigated the immunological and genetic profiles of two patients with metastatic melanoma and one patient affected by lung cancer, who developed severe psoriasis after receiving anti-PD-1 nivolumab therapy.
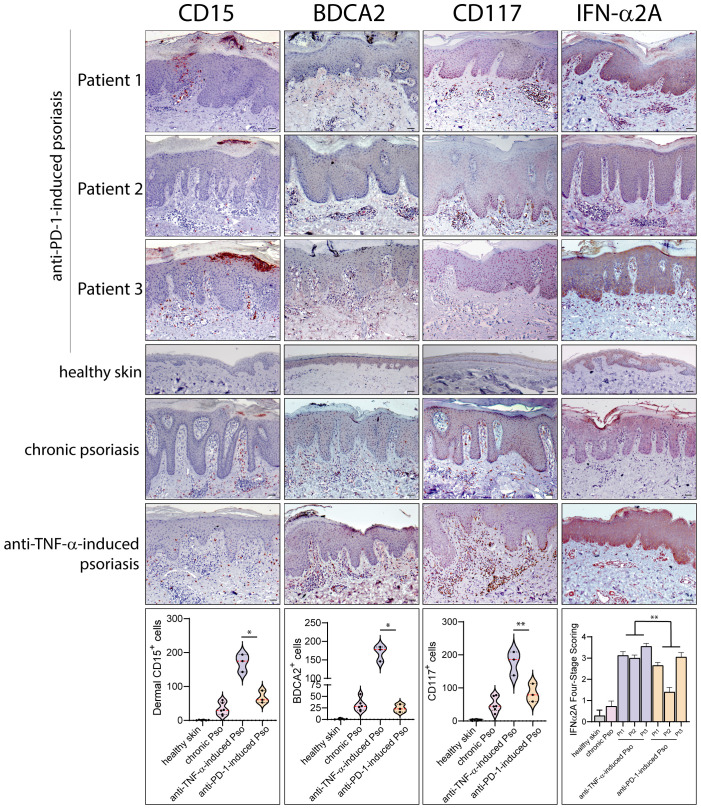
Methods: The immune patterns of the three patients were compared with those detectable in classical, chronic plaque-type psoriasis or paradoxical psoriasis induced by anti-TNF-α therapy, mostly sustained by adaptive and innate immunity processes, respectively. Therefore, immunohistochemistry and mRNA analyses of innate and adaptive immunity molecules were conducted on skin biopsy of patients. Genetic analysis of polymorphisms predisposing to psoriasis was carried out by NGS technology.
Results: We found that anti-PD-1-induced psoriasis showed immunological features similar to chronic psoriasis, characterized by the presence of cellular players of adaptive immunity, with abundant CD3+, CD8+ T cells and CD11c+ dendritic cells infiltrating skin lesions, and producing IL-23, IL-6, TNF-α, IFN-γ and IL-17. On the contrary, a lower number of innate immunity cells (BDCA2+ plasmacytoid dendritic cells, CD15+ neutrophils, CD117+ mast cells) and reduced IFN-α/β, lymphotoxin (LT)-α/β, were observed in anti-PD-1-induced psoriasis lesions, as compared with anti-TNF-α-induced paradoxical psoriasis. Importantly, the disintegrin and metalloprotease domain containing thrombospondin type 1 motif-like 5 (ADAMTSL5) psoriasis autoantigen was significantly upregulated in psoriasis lesions of anti-PD-1-treated patients, at levels comparable with chronic plaque-type psoriasis. Finally, NGS analysis revealed that all patients carried several allelic variants in psoriasis susceptibility genes, such as HLA-C, ERAP1 and other genes of the major psoriasis susceptibility PSORS1 locus.
Discussion: Our study showed that adaptive immunity predominates over innate immunity in anti-PD-1-induced psoriasis lesions, consistently with the local ADAMTSL5 overexpression. The presence of numerous SNPs in psoriasis susceptibility genes of the three patients also suggested their strong predisposition to the disease.
Keywords: adaptive immunity; anti-PD-1 therapy; immune-related cutaneous adverse event (ircAE); innate immunity; melanoma; paradoxical skin reactions; psoriasis.
Copyright © 2024 Morelli, Carbone, Scaglione, Scarponi, Di Francesco, Pallotta, De Galitiis, Rahimi, Madonna, Failla and Albanesi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
-
- Xing P, Zhang F, Wang G, Xu Y, Li C, Wang S, et al. . Incidence rates of immune-related adverse events and their correlation with response in advanced solid tumours treated with NIVO or NIVO+IPI: a systematic review and meta-analysis. J Immunother Cancer. (2019) 7:341–50. doi: 10.1186/s40425-019-0779-6 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous