

Estimating maximum work rate during cardiopulmonary exercise testing from the six-minute walk distance in patients with heart failure
- PMID: 38496329
- PMCID: PMC10943044
- DOI: 10.1016/j.ijcrp.2024.200247
Estimating maximum work rate during cardiopulmonary exercise testing from the six-minute walk distance in patients with heart failure
Abstract
Background: Exercise is recommended for patients with chronic heart failure (CHF) and its intensity is usually set as a percentage of the maximal work rate (MWR) during cardiopulmonary exercise testing (CPX) or a symptom-limited incremental test (SLIT). As these tests are not always available in cardiac rehabilitation due to logistic/cost constraints, we aimed to develop a predictive model to estimate MWR at CPX (estMWR@CPX) in CHF patients using anthropometric and clinical measures and the 6-min walk test (6 MWT), the most widely used exercise field test.
Methods: This is a multicentre cross-sectional retrospective study in a cardiac rehabilitation setting. Six hundred patients with HF in New York Heart Association (NYHA) functional class I-III underwent both CPX and 6 MWT and, through multivariable linear regression analysis, we defined several predictive models to define estMWR@CPX.
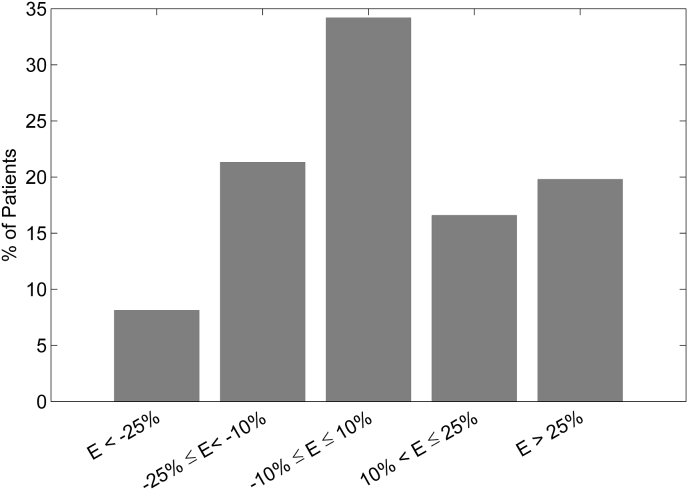
Results: The best model included 6 MWT, sex, age, weight, NYHA class, left ventricular ejection fraction (LVEF), smoking status and chronic obstructive pulmonary disease COPD (adjusted R2 = 0.55; 95% LoA -39 to 33 W). When LVEF was excluded as a predictor, the resulting model performed only slightly worse (adjusted R2 = 0.54; 95% LoA -42 to 34 W). Only in 34% of cases was the percentage difference between estMWR@CPX and real MWR@CPX <10% in absolute value. EstMWR@CPX tended to overestimate low values and underestimate high values of true MWR@CPX.
Conclusions: Our results showed a lack of accuracy in the predictive model evaluated; therefore, for an accurate prescription of cycle-ergometer exercise training, it is necessary to assess MWR by CPX or SLIT.
Keywords: 6-Min walking test; Cardiopulmonary exercise testing; Chronic heart failure.
© 2024 The Authors.
Conflict of interest statement
All Authors declare no conflict of interest relevant to the research, analysis, or interpretation presented in the manuscript.
Figures

Similar articles
-
A moderate 500-m treadmill walk for estimating peak oxygen uptake in men with NYHA class I-II heart failure and reduced left ventricular ejection fraction.BMC Cardiovasc Disord. 2018 Apr 16;18(1):67. doi: 10.1186/s12872-018-0801-9. BMC Cardiovasc Disord. 2018. PMID: 29661150 Free PMC article.
-
Monitoring of ventilation during the early part of cardiopulmonary exercise testing: the first step to detect central sleep apnoea in chronic heart failure.Sleep Med. 2008 May;9(4):411-7. doi: 10.1016/j.sleep.2007.06.012. Epub 2007 Aug 29. Sleep Med. 2008. PMID: 17761455
-
6-min walk test provides prognostic utility comparable to cardiopulmonary exercise testing in ambulatory outpatients with systolic heart failure.J Am Coll Cardiol. 2012 Dec 25;60(25):2653-61. doi: 10.1016/j.jacc.2012.08.1010. Epub 2012 Nov 21. J Am Coll Cardiol. 2012. PMID: 23177293 Free PMC article. Clinical Trial.
-
[The 6 minute walking test: a cost-effective alternative to spiro-ergometry in patients with chronic heart failure?].Z Kardiol. 2000 Feb;89(2):72-80. doi: 10.1007/s003920050012. Z Kardiol. 2000. PMID: 10768274 Review. German.
-
Ivabradine Improves Cardiac Function and Increases Exercise Capacity in Patients with Chronic Heart Failure.Int Heart J. 2019 Jul 27;60(4):899-909. doi: 10.1536/ihj.18-559. Epub 2019 Jul 12. Int Heart J. 2019. PMID: 31308326
Cited by
-
Evaluating the Efficacy of Coronary Sinus Reducer Implantation in the Management of Refractory Angina: A Systematic Review and Meta-Analysis.Cureus. 2024 Jul 29;16(7):e65662. doi: 10.7759/cureus.65662. eCollection 2024 Jul. Cureus. 2024. PMID: 39205733 Free PMC article. Review.
-
Oxygen uptake efficiency plateau is unaffected by fitness level - the NOODLE study.BMC Sports Sci Med Rehabil. 2024 Jul 10;16(1):151. doi: 10.1186/s13102-024-00939-w. BMC Sports Sci Med Rehabil. 2024. PMID: 38987830 Free PMC article.
References
-
- Taylor R.S., Long L., Mordi I.R., et al. Exercise-based rehabilitation for heart failure: Cochrane systematic review, Meta-analysis, and Trial Sequential analysis. JACC Heart Fail. 2019;7:691–705. - PubMed
-
- Authors/Task Force Members. McDonagh T.A., Metra M., Adamo M., et al. ESC Scientific Document Group 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2022;24:4–131. - PubMed
-
- Mezzani A., Hamm L.F., Jones A.M., et al. European association for cardiovascular prevention and rehabilitation; American association of cardiovascular and pulmonary rehabilitation; Canadian association of cardiac rehabilitation aerobic exercise intensity assessment and prescription in cardiac rehabilitation: a joint position statement of the European association for cardiovascular prevention and rehabilitation, the American association of cardiovascular and pulmonary rehabilitation and the Canadian association of cardiac rehabilitation. Eur J Prev Cardiol. 2013;20:442–467. - PubMed
-
- Shoemaker M.J., Dias K.J., Lefebvre K.M., Heick J.D., Collins S.M. Physical therapist clinical practice guideline for the Management of Individuals with heart failure. Phys. Ther. 2020;100:14–43. - PubMed
-
- Task Force of the Italian Working Group on Cardiac Rehabilitation and Prevention (Gruppo Italiano di Cardiologia Riabilitativa e Prevenzione, GICR) Working Group on Cardiac Rehabilitation and Exercise Physiology of the European Society of Cardiology Statement on cardiopulmonary exercise testing in chronic heart failure due to left ventricular dysfunction: recommendations for performance and interpretation Part III: interpretation of cardiopulmonary exercise testing in chronic heart failure and future applications. Eur. J. Cardiovasc. Prev. Rehabil. 2006;13:485–494. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous