

Case Reports
doi: 10.1016/j.hrcr.2023.12.005.
eCollection 2024 Mar.
Right bundle branch activation during left bundle branch pacing: Marginal gains in left bundle branch pacing-optimized cardiac resynchronization therapy and the effects of atrioventricular delay dynamic optimization
Affiliations
- PMID: 38496735
- PMCID: PMC10943543
- DOI: 10.1016/j.hrcr.2023.12.005
Item in Clipboard
Case Reports
Right bundle branch activation during left bundle branch pacing: Marginal gains in left bundle branch pacing-optimized cardiac resynchronization therapy and the effects of atrioventricular delay dynamic optimization
HeartRhythm Case Rep.
.
No abstract available
Keywords: Cardiac resynchronization; Left bundle branch pacing (LBBP); Noninvasive programmed electrical stimulation; Right bundle branch activation; SyncAV.
Conflict of interest statement
The authors do not have any conflict of interest to declare.
Figures
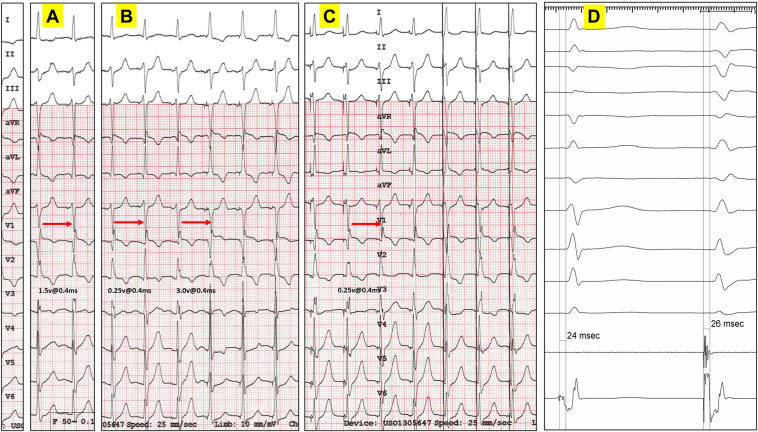
Bipolar and unipolar threshold testing post implantation. A: The first transition occurred at an output of 1.5 V @ 0.4 ms, corresponding with nonselective left bundle branch pacing (ns-LBBP) and anodal loss of capture (note a change in lead V1 from a Qr to a QR pattern). B: As output is further decreased, there is a second transition from a QR pattern to a qR pattern in lead V1, with an isoelectric interval, at an output of 0.25 V @ 0.4 ms corresponding with transition from ns-LBBP to selective (s)-LBBP, followed by the last 3 beats with a Qr pattern (safety pacing at nominal output 3.0 V @ 0.4 ms, ns-LBBP and anodal capture). C: Only 1 transition occurred at low output (anodal capture is not possible). In lead V1, transition from a QR pattern to a qR pattern with an isoelectric interval was noted at an output of 0.25 V @ 0.4 ms, corresponding with transition from ns-LBBP to s-LBBP, followed by the last 3 beats with a similar QR pattern (safety pacing at nominal output 3.0 V @ 0.4 ms, ns-LBBP without anodal capture). D: Left bundle branch potential (Po LBB) was demonstrated at implant. A similar interval was noted between Po LBB to QRS and stim-QRS with s-LBBP.
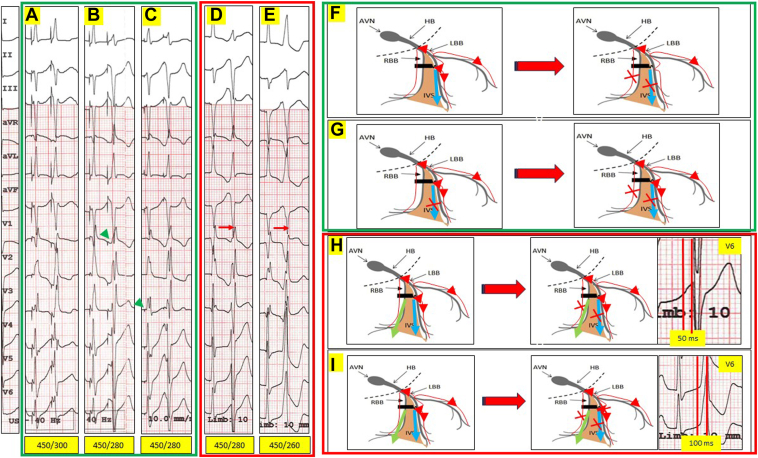
Unipolar and bipolar noninvasive programmed electrical stimulation (NIPS) using the implanted device. A drive train of 8 pulses was delivered at a cycle length (CL) of 450 ms (sinus CL was 550 ms), followed by S2 at 20 ms decrements. A,B: Unipolar NIPS output of 2.5 V @ 0.4 ms (nonselective left bundle branch pacing [ns-LBBP] without anodal capture). NIPS at 450/280 ms resulted in a change in morphology and an isoelectric line between the stimulation spike and QRS. The right bundle branch (RBB) and left ventricular (LV) septum in this instance have a similar effective refractory period (ERP). As a result, the extrastimuli S2 resulted in selective (s)-LBBP and RBB block (RBBB), with a clear isoelectric interval between stim to QRS (green arrowhead). (This is represented schematically in panel F). C: Unipolar NIPS output of 0.75 V @ 0.1 ms (consistent s-LBBP without anodal capture). An isoelectric interval was noted between the stimulus spike and the QRS with a qR pattern in V1 during the drive train. NIPS at 450/280 ms resulted in a change in morphology (similar RBBB morphology as in panel B; s-LBBP and RBBB). The qR pattern during s-LBBP is narrower (incomplete RBBB pattern), as there is retrograde conduction from the LBBP site and activation of the RBB via transverse interconnections. Conduction would be slower (hence a broader QRS) compared to normal conduction whereby both the RBB and the left bundle branch (LBB) are activated simultaneously from the atrioventricular node (AVN). (This is represented schematically in panel G). D: Bipolar NIPS at output of 2.5 V @ 0.4 ms (consistent ns-LBBP with anodal capture). NIPS at 450/280 ms resulted in a change in morphology (RBBB morphology; s-LBBP, RBBB, and anodal RV septal capture). In this instance, anodal RV septal capture ERP is greater than the RBB and LV septal cathodal ERP. The LBB continues to be captured, as evidenced by the short V6 R-wave peak time (V6RWPT) of 50 ms. (This is represented schematically in panel H). E: Bipolar NIPS at output of 2.5 V @ 0.4 ms (consistent ns-LBBP with anodal capture). NIPS at 450/260 ms resulted in another change in morphology in lead V1 (a LBBB morphology, Qr pattern; anodal RV septal capture alone, LBB ERP reached). The V6RWPT is now prolonged at 100 ms. (This is represented schematically in panel I). Blue arrows indicate cathodal LV septal capture; green arrows indicate anodal RV septal capture. HB = His bundle; IVS = interventricular septum.
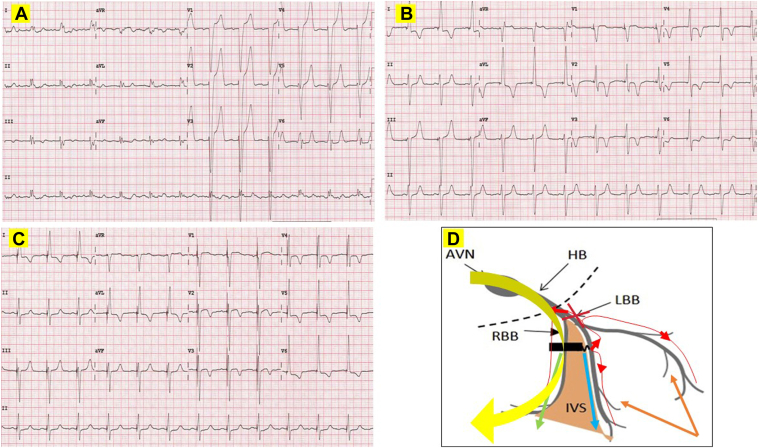
Baseline, postimplant left bundle branch pacing–optimized cardiac resynchronization therapy (LOT-CRT) and postimplant SyncAV LOT-CRT electrocardiogram (ECG). A: Baseline ECG for patient 2 showing normal sinus rhythm at a rate of 74 beats/min and left bundle branch (LBB) block. QRS duration of 170 ms, notching in leads I and aVL, QS pattern in leads V1 and aVR, and V6 R-wave peak time of 80 ms. B: Postimplant LOT-CRT ECG. Pacing in DDD mode with a short 80 ms atrioventricular (AV) delay. Left bundle branch pacing (LBBP) at an output of 2.5 V @ 0.4 ms (nonselective LBBP [ns-LBBP] and anodal capture) with an offset of +15 ms is followed by epicardial anterior lateral left ventricular (LV) pacing via the coronary sinus (CS) lead (M3-RV coil vector) demonstrated the narrowest fused QRS duration of 120 ms. C: Postimplant LOT-CRT final ECG. LBBP at an output of 2.5 V @ 0.4 ms (ns-LBBP and anodal capture) with an offset of +15 ms is followed by epicardial anterior-lateral LV pacing via the CS lead (vector: M3-RV coil). Sensed AV delay at baseline was measured at 250 ms. SyncAV delta of -80 ms resulted in further narrowing of the QRS to 100 ms. D: Schematic representation of likely activation wavefronts. The LV conduction abnormalities were corrected by a combination of (1) ns-LBBP (left bundle branch [LBB] capture and cathodal LV septal capture: QRS narrowed from 170 ms to 140 ms), and LV epicardial pacing via the CS lead (further shortening QRS from 140 ms to 120 ms). There is proximal LBB complete conduction block. SyncAV prolongs biventricular pacing AV duration dynamically, allowing for normal AV nodal conduction down the nondiseased right bundle branch (RBB), further shortening of the QRS to 10 ms. Blue arrow: cathodal LV septal capture; green arrow: anodal RV septal capture; yellow arrow: AV nodal conduction down the RBB with SyncAV; brown arrows: LV epicardial activation from the CS lead. AVN = atrioventricular node; HB = His bundle; IVS = interventricular septum.
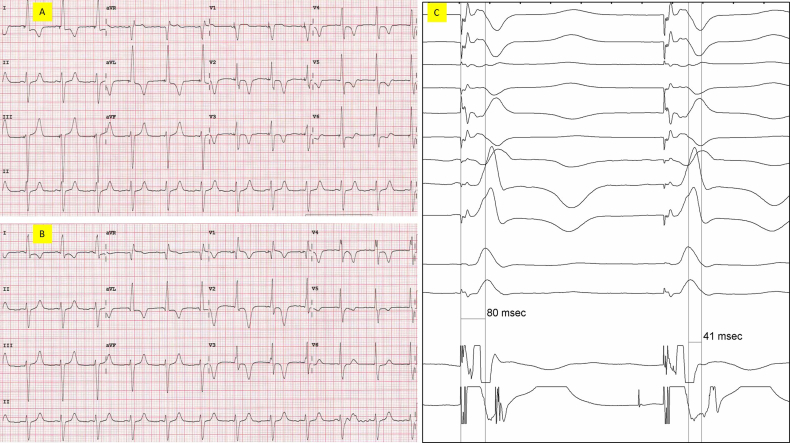
A) Post implant bipolar LBBP at an output of 2.5v@0.4ms demonstrating ns-LBBP with anodal capture. QS in V1, QRS duration 140ms, and V6RWPT 80ms. B) Post implant bipolar LBBP at an output of 1.0v@0.4ms demonstrating ns-LBBP without anodal capture. QR in V1, minimal change QRS duration, and V6RWPT remains at 80ms. C) Bipolar LBBP at an output of 2.5v@0.4ms demonstrating a V6RWPT of 80ms, and a V6-V1 interpeak of 40ms.
Similar articles
-
Electrocardiographic imaging demonstrates electrical synchrony improvement by dynamic atrioventricular delays in patients with left bundle branch block and preserved atrioventricular conduction.Europace. 2023 Feb 16;25(2):536-545. doi: 10.1093/europace/euac224. Europace. 2023. PMID: 36480445 Free PMC article.
-
Programming Cardiac Resynchronization Therapy for Electrical Synchrony: Reaching Beyond Left Bundle Branch Block and Left Ventricular Activation Delay.J Am Heart Assoc. 2018 Feb 6;7(3):e007489. doi: 10.1161/JAHA.117.007489. J Am Heart Assoc. 2018. PMID: 29432133 Free PMC article.
-
Stepwise application of ECG and electrogram-based criteria to ensure electrical resynchronization with left bundle branch pacing.Europace. 2023 Jun 2;25(6):euad128. doi: 10.1093/europace/euad128. Europace. 2023. PMID: 37294671 Free PMC article. Clinical Trial.
-
Left bundle branch pacing in heart failure patients with left bundle branch block: A systematic review and meta-analysis.Pacing Clin Electrophysiol. 2022 Feb;45(2):212-218. doi: 10.1111/pace.14405. Epub 2022 Jan 17. Pacing Clin Electrophysiol. 2022. PMID: 34766359
-
Left Bundle Branch Pacing: Current Knowledge and Future Prospects.Front Cardiovasc Med. 2021 Mar 23;8:630399. doi: 10.3389/fcvm.2021.630399. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 33834042 Free PMC article. Review.
References
-
- Huang W., Su L., Wu S., et al. A novel pacing strategy with low and stable output: pacing the left bundle branch immediately beyond the conduction block. Can J Cardiol. 2017;33:1736.e1–1736.e3. - PubMed
-
- Hua W., Fan X., Li X., et al. Comparison of left bundle branch and His bundle pacing in bradycardia patients. JACC Clin Electrophysiol. 2020;6:1291–1299. - PubMed
-
- Vijayaraman P., Subzposh F.A., Naperkowski A., et al. Prospective evaluation of feasibility and electrophysiologic and echocardiographic characteristics of left bundle branch area pacing. Heart Rhythm. 2019;16:1774–1782. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
