

Cardiac paraganglioma: implications and impacts of a rare disease-a case report †
- PMID: 38496798
- PMCID: PMC10941256
- DOI: 10.1093/ehjcr/ytae032
Cardiac paraganglioma: implications and impacts of a rare disease-a case report †
Abstract
Background: Tumour-producing catecholamines arise in the adrenal medulla (pheochromocytomas), as well as in extra-adrenal chromaffin cells (paragangliomas). The origin can be from any location; however, it is very rare in the heart.
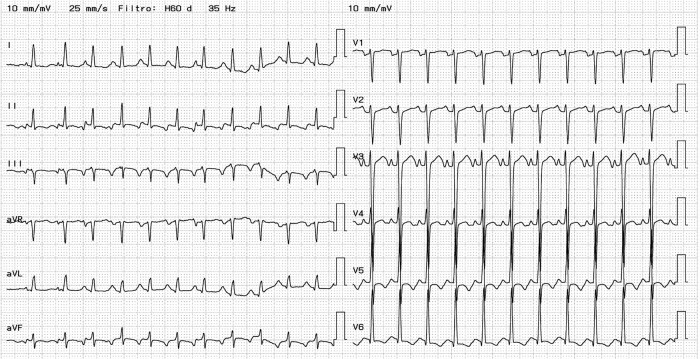
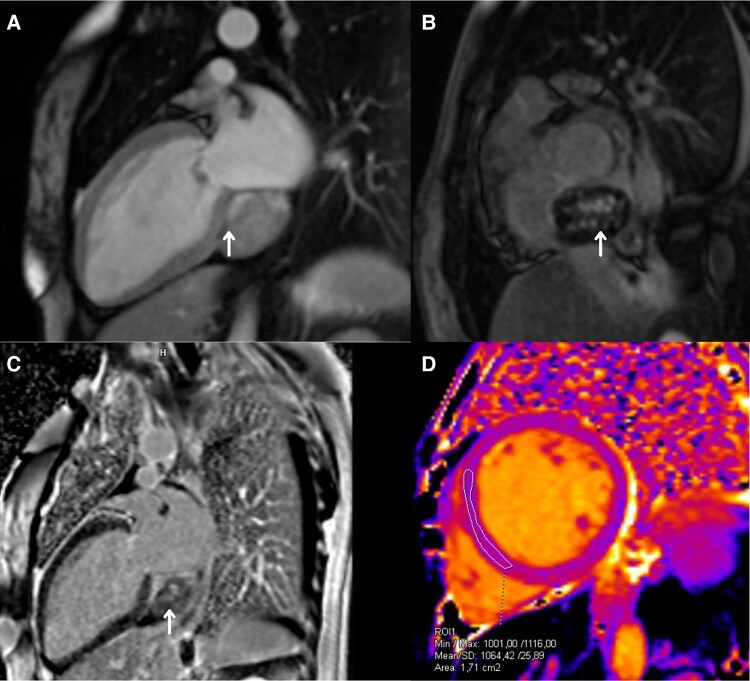
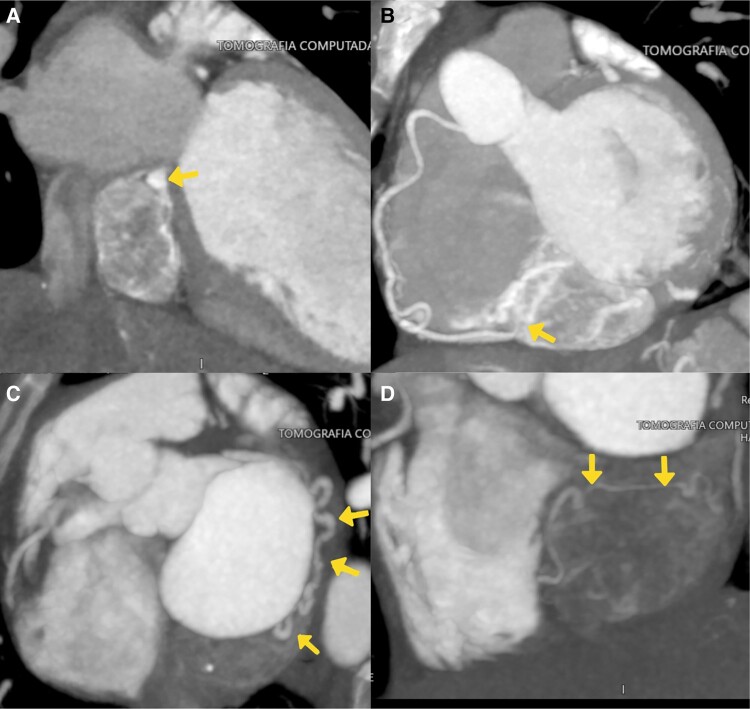
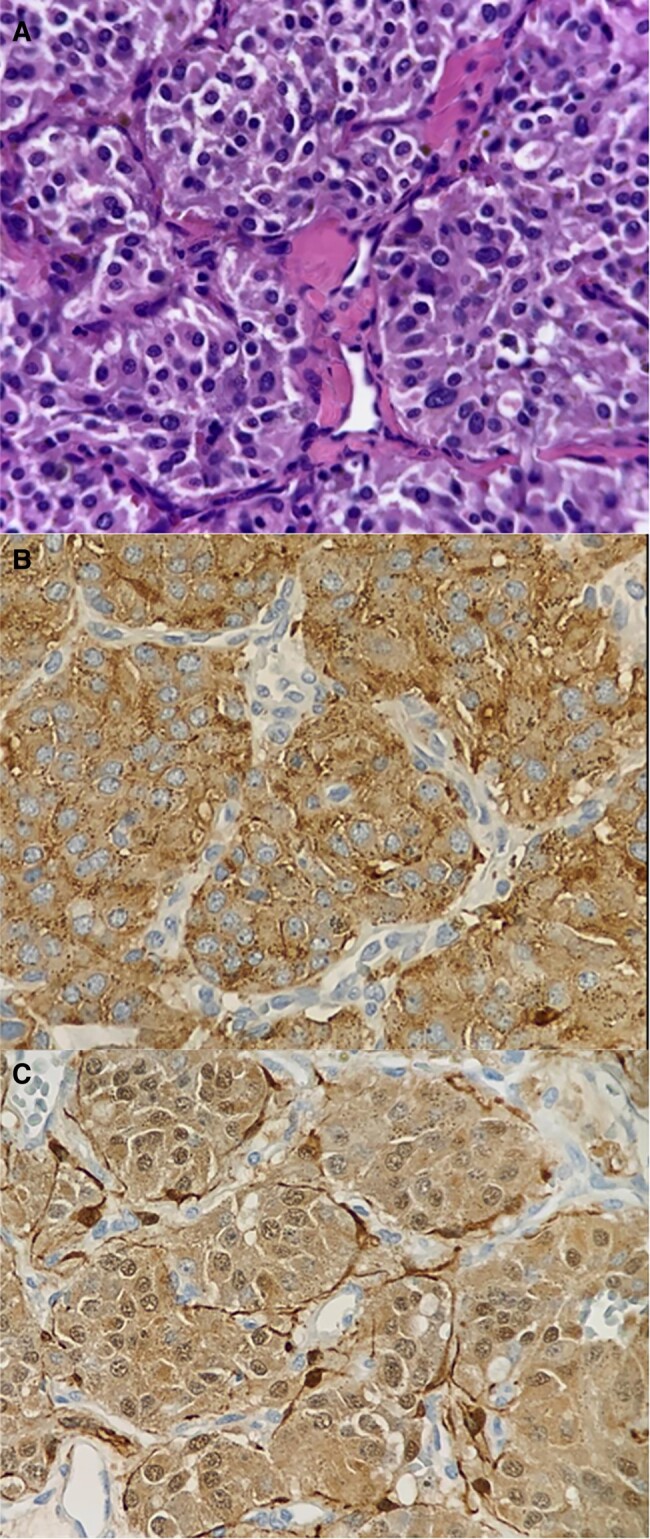
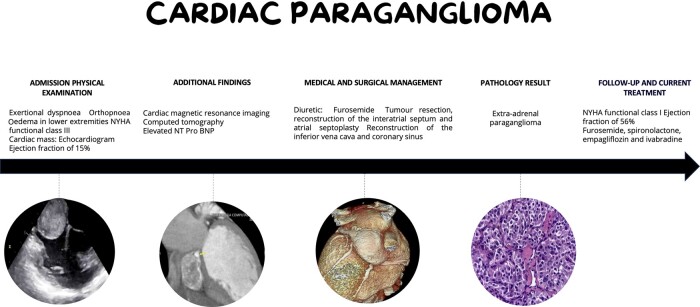
Case summary: A 43-year-old woman with a history of arterial hypertension presented with dyspnoea on moderate exertion, New York Class Association (NYHA) functional classes III and IV, and oedema in the lower extremities. Medical and laboratory evaluation revealed an NT-proBNP of 6046 pg/mL, a left ventricular ejection fraction (LVEF) of 15%, longitudinal strain of -7%, and a mass located on the inner surface of the left atrioventricular groove. Surgical intervention was performed, and the tumour was resected. Pathological report showed an extra-adrenal paraganglioma without neoplastic involvement in the margins of the vena cava. After surgery, the patient showed clinical improvement with NYHA functional class I, LVEF of 56%, and longitudinal strain of -20% on transthoracic echocardiography 4 months after treatment.
Discussion: Paragangliomas are tumours that are rarely found in the heart, and their diagnosis is difficult. However, early detection and treatment can improve the quality of life of affected patients.
Keywords: Cardiac tumour; Case report; Catecholamines; Dilated cardiomyopathy; Heart failure; Paraganglioma.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures

Similar articles
-
A rare case report of ectopic-adrenal paraganglioma with inferior vena cava infiltration. Case report and literature review.Int J Surg Case Rep. 2024 Feb;115:109315. doi: 10.1016/j.ijscr.2024.109315. Epub 2024 Feb 1. Int J Surg Case Rep. 2024. PMID: 38306874 Free PMC article.
-
[Association of plasma amino-terminal pro-A-, B- and C-type natriuretic peptide levels with NYHA grade and echocardiographic derived parameters of cardiac function in heart failure patients].Zhonghua Xin Xue Guan Bing Za Zhi. 2009 Jun;37(6):486-90. Zhonghua Xin Xue Guan Bing Za Zhi. 2009. PMID: 19927626 Chinese.
-
Catecholamine-induced cardiomyopathy improvement after para-aortic paraganglioma resection: a case report.ESC Heart Fail. 2022 Feb;9(1):213-218. doi: 10.1002/ehf2.13783. Epub 2021 Dec 29. ESC Heart Fail. 2022. PMID: 34967117 Free PMC article.
-
Giant Paraganglioma Complicated With Catecholamine Crisis and Catecholamine Cardiomyopathy: A Case Report and Review of the Literature.Front Endocrinol (Lausanne). 2022 Feb 3;12:790080. doi: 10.3389/fendo.2021.790080. eCollection 2021. Front Endocrinol (Lausanne). 2022. PMID: 35185782 Free PMC article. Review.
-
A rare case of multiple paragangliomas in the head and neck, retroperitoneum and duodenum: A case report and review of the literature.Front Endocrinol (Lausanne). 2023 Jan 10;13:1054468. doi: 10.3389/fendo.2022.1054468. eCollection 2022. Front Endocrinol (Lausanne). 2023. PMID: 36704041 Free PMC article. Review.
Cited by
-
Familial Paraganglioma Presenting With Acute Coronary Syndrome and Coronary Vasospasm.JCEM Case Rep. 2025 Apr 18;3(6):luaf082. doi: 10.1210/jcemcr/luaf082. eCollection 2025 Jun. JCEM Case Rep. 2025. PMID: 40255443 Free PMC article.
References
-
- Kapetanakis S, Chourmouzi D, Gkasdaris G, Katsaridis V, Eleftheriadis E, Givissis P. Functional extra-adrenal paraganglioma of the retroperitoneum giving thoracolumbar spine metastases after a five-year disease-free follow-up: a rare malignant condition with challenging management. Pan Afr Med J 2017;28:94. - PMC - PubMed
-
- Chan EY, Ali A, Umana JP, Nguyen DT, Hamilton DJ, Graviss EA, et al. Management of primary cardiac paraganglioma. J Thorac Cardiovasc Surg 2022;164:158–166.e1. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials