

Comparison of Normocalcemic vs Hypercalcemic Primary Hyperparathyroidism in a Hypercalciuric Renal Stone Population
- PMID: 38497124
- PMCID: PMC11403309
- DOI: 10.1210/clinem/dgae162
Comparison of Normocalcemic vs Hypercalcemic Primary Hyperparathyroidism in a Hypercalciuric Renal Stone Population
Abstract
Context: Primary hyperparathyroidism (PHPT) is commonly diagnosed in the setting of hypercalcemia, whereas normocalcemic primary hyperparathyroidism (NHPT) may be misdiagnosed.
Objective: Our objective was to compare patients with hypercalcemic hyperparathyroidism (HPHPT) vs patients with NHPT hypercalciuric renal stones.
Methods: We took advantage of a routine calcium load test performed in patients with hypercalciuric renal stones to assess retrospectively among patients with PHPT the prevalence and characteristics of NHPT and HPHPT under a calcium-restricted diet.
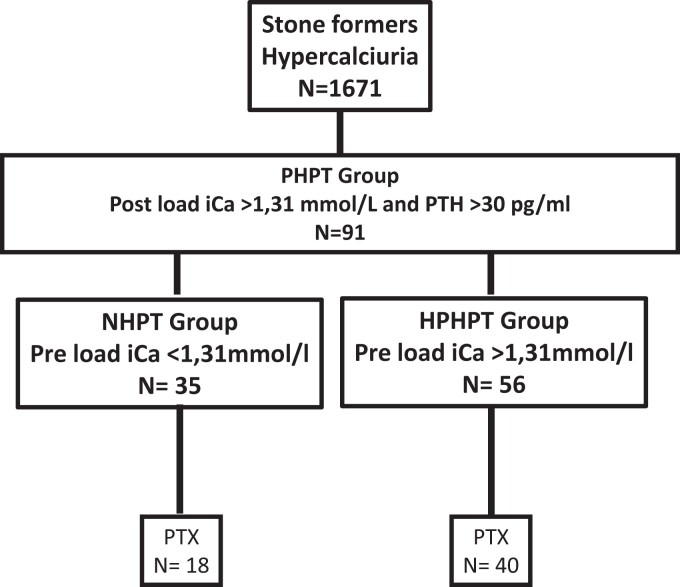
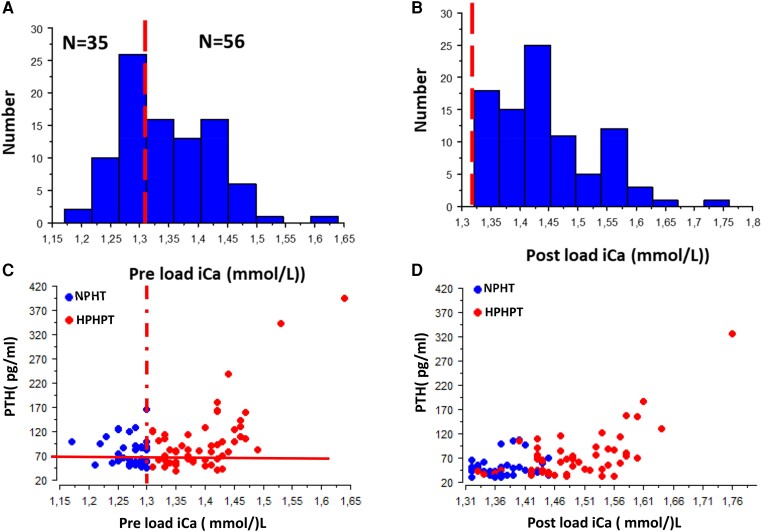
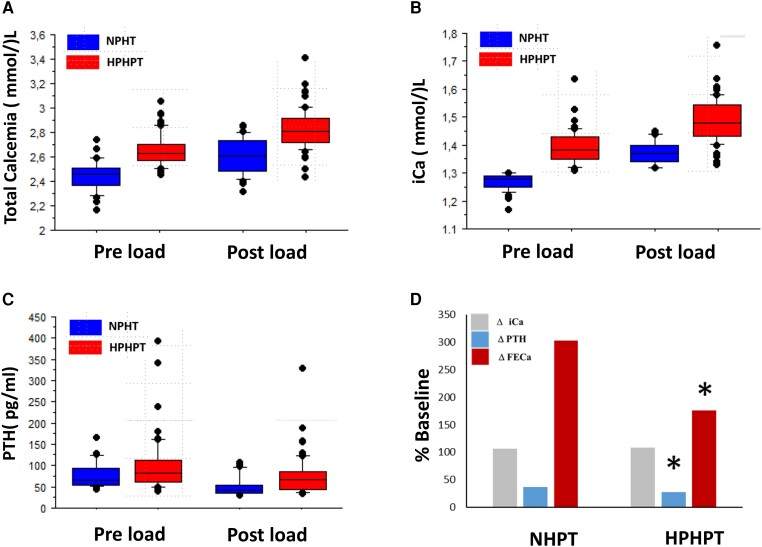
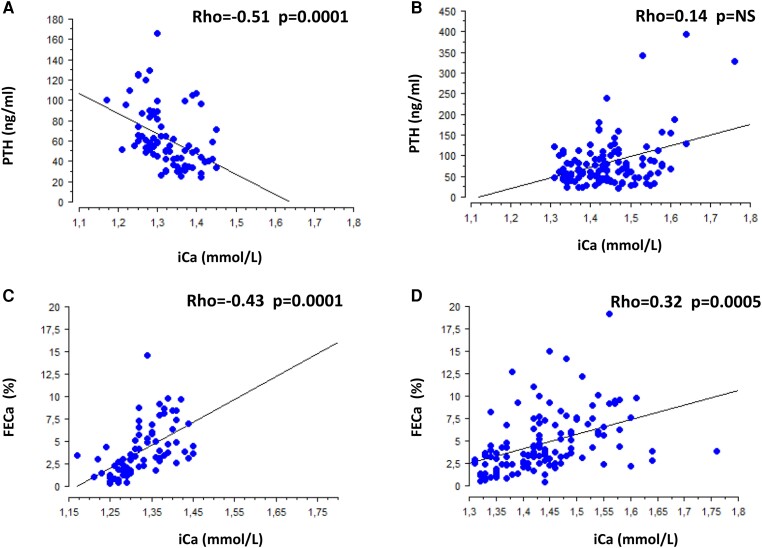
Results: Among 1671 patients with hypercalciuria, 91 patients had a final diagnosis of PHPT (postload ionized calcium [iCa] > 1.31 mmol/L and parathyroid hormone [PTH] > 30 pg/mL). Prevalence of NHPT is 40% of all PHPT; however, according to total serum calcium, 4/35 NHPT and 7/56 HPHPT cases would have been misclassified in the other group. Eighteen of 35 NHPT and 40/56 HPHPT cases underwent parathyroidectomy. No significant characteristics relating to parathyroid weight, stone composition, or bone remodeling biomarkers were detected between groups. Although iCa is higher in HPHPT in the fasting state and after calcium load, we found no difference for calcium diet, 24-hour calciuria, or calcitriol. Renal calcium excretion postload increased by 303% in NHPT but only 176% in HPHPT (P = .01) likely explained by a lesser PTH decrease (P = .02). However, a strong negative association (P < .0001) detected between pooled preload and postload iCa and PTH only in the NHPT group suggests a persistent efficient PTH-CaSR control within the parathyroid glands in this group.
Conclusion: Our data show the relevance of dynamic tests to unmask NHPT in patients with hypercalciuric renal stones.
Keywords: CaSR; hypercalcemic primary hyperparathyroidism; hypercalciuria; normocalcemic primary hyperparathyroidism; primary hyperparathyroidism.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
-
- Bilezikian JP, Khan AA, Silverberg SJ, et al. Evaluation and management of primary hyperparathyroidism: summary statement and guidelines from the fifth international workshop. J Bone Miner Res. 2022;37(11):2293‐2314. - PubMed
-
- Maruani G, Hertig A, Paillard M, Houillier P. Normocalcemic primary hyperparathyroidism: evidence for a generalized target-tissue resistance to parathyroid hormone. J Clin Endocrinol Metab. 2003;88(10):4641‐4648. - PubMed
-
- Siprova H, Frysak Z, Soucek M. Primary hyperparathyroidism, with a focus on management of the normocalcemic form: to treat or not to treat? Endocr Pract. 2016;22(3):294‐301. - PubMed
-
- Souberbielle JC, Cavalier E, Cormier C. How to manage an isolated elevated PTH? Ann Endocrinol (Paris). 2015;76(2):134‐141. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
