

Value of multiplanar reconstruction in multi-slice computed tomography for the detection of foreign body in the pulmonary artery: a case report
- PMID: 38497130
- PMCID: PMC10946078
- DOI: 10.1177/03000605241237890
Value of multiplanar reconstruction in multi-slice computed tomography for the detection of foreign body in the pulmonary artery: a case report
Abstract
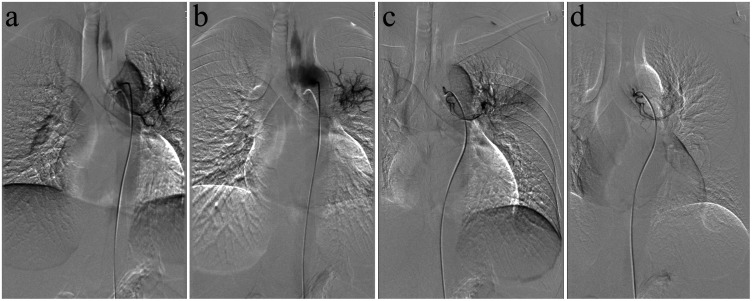
Multi-slice computed tomography (MSCT) is the primary method for the detection and visualization of foreign bodies in the pulmonary artery because it provides high sensitivity and accuracy. It is very difficult to diagnose a patient with a non-iatrogenic pulmonary artery foreign body who does not have a history of a penetrating trauma. This case report describes a 36-year-old male that presented with coughing and haemoptysis. Based on conventional coronal and cross-sectional CT, the foreign body was misdiagnosed as pulmonary tuberculosis and pulmonary artery thrombosis. During treatment of the bronchial artery embolization and anti-tuberculosis therapy, the patient continued to experience haemoptysis. After further analysis of the pulmonary artery CT angiography images and curved multiplane reconstruction, an approximately 6-cm long toothpick was identified in the pulmonary artery with an unclear entry route. After surgery to remove the toothpick, symptoms of coughing and haemoptysis were resolved. This current case demonstrated that multiplane reconstruction in MSCT can improve the detection and visualization of pulmonary artery foreign bodies, which can aid in the diagnosis of pulmonary artery diseases of unknown cause.
Keywords: Foreign body; computed tomography; multiplane reconstruction; pulmonary artery.
Conflict of interest statement
Declaration of conflicting interestThe authors declare that there are no conflicts of interest.
Figures





Similar articles
-
A strange case of foreign body embolism in the right lower pulmonary artery.Gen Thorac Cardiovasc Surg. 2021 May;69(5):894-896. doi: 10.1007/s11748-020-01570-5. Epub 2021 Jan 5. Gen Thorac Cardiovasc Surg. 2021. PMID: 33400199 Free PMC article.
-
[A rare cause of hemoptysis].Rev Pneumol Clin. 1999 Mar;55(1):35-7. Rev Pneumol Clin. 1999. PMID: 10367314 French.
-
[Severe haemoptysis revealing a Rasmüssen aneurysm].Rev Mal Respir. 2010;27(1):63-6. doi: 10.1016/j.rmr.2009.11.009. Epub 2009 Dec 14. Rev Mal Respir. 2010. PMID: 20146953 French.
-
Radiologic management of haemoptysis: diagnostic and interventional bronchial arterial embolisation.Rofo. 2015 Apr;187(4):248-59. doi: 10.1055/s-0034-1385457. Epub 2014 Nov 5. Rofo. 2015. PMID: 25372159 Review.
-
A case of bronchial Dieulafoy disease and literature review.J Cardiothorac Surg. 2023 Jun 27;18(1):197. doi: 10.1186/s13019-023-02279-1. J Cardiothorac Surg. 2023. PMID: 37370170 Free PMC article. Review.
References
-
- Gagnier JJ, Kienle G, Altman DG, et al.. The CARE guidelines: consensus-based clinical case reporting guideline development. Headache 2013; 53: 1541–1547. - PubMed
-
- Goodwin RA, Des Prez RM. Apical localization of pulmonary tuberculosis, chronic pulmonary histoplasmosis, and progressive massive fibrosis of the lung. Chest 1983; 83: 801–805. - PubMed
-
- Qu PF, Bai BL, Duan T, et al.. Multiple Pulmonary Infarction and Abscess Caused by a Bamboo Stick Accidentally Piercing into Chest: a Case Misdiagnosed as Pulmonary Tuberculosis. Chin Med Sci J 2021; 252–256. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
