

Neurodevelopmental Outcomes of Extremely Preterm Infants Fed Donor Milk or Preterm Infant Formula: A Randomized Clinical Trial
- PMID: 38497706
- PMCID: PMC10828950
- DOI: 10.1001/jama.2023.27693
Neurodevelopmental Outcomes of Extremely Preterm Infants Fed Donor Milk or Preterm Infant Formula: A Randomized Clinical Trial
Abstract
Importance: Maternal milk feeding of extremely preterm infants during the birth hospitalization has been associated with better neurodevelopmental outcomes compared with preterm formula. For infants receiving no or minimal maternal milk, it is unknown whether donor human milk conveys similar neurodevelopmental advantages vs preterm formula.
Objective: To determine if nutrient-fortified, pasteurized donor human milk improves neurodevelopmental outcomes at 22 to 26 months' corrected age compared with preterm infant formula among extremely preterm infants who received minimal maternal milk.
Design, setting, and participants: Double-blind, randomized clinical trial conducted at 15 US academic medical centers within the Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Infants younger than 29 weeks 0 days' gestation or with a birth weight of less than 1000 g were enrolled between September 2012 and March 2019.
Intervention: Preterm formula or donor human milk feeding from randomization to 120 days of age, death, or hospital discharge.
Main outcomes and measures: The primary outcome was the Bayley Scales of Infant and Toddler Development (BSID) cognitive score measured at 22 to 26 months' corrected age; a score of 54 (score range, 54-155; a score of ≥85 indicates no neurodevelopmental delay) was assigned to infants who died between randomization and 22 to 26 months' corrected age. The 24 secondary outcomes included BSID language and motor scores, in-hospital growth, necrotizing enterocolitis, and death.
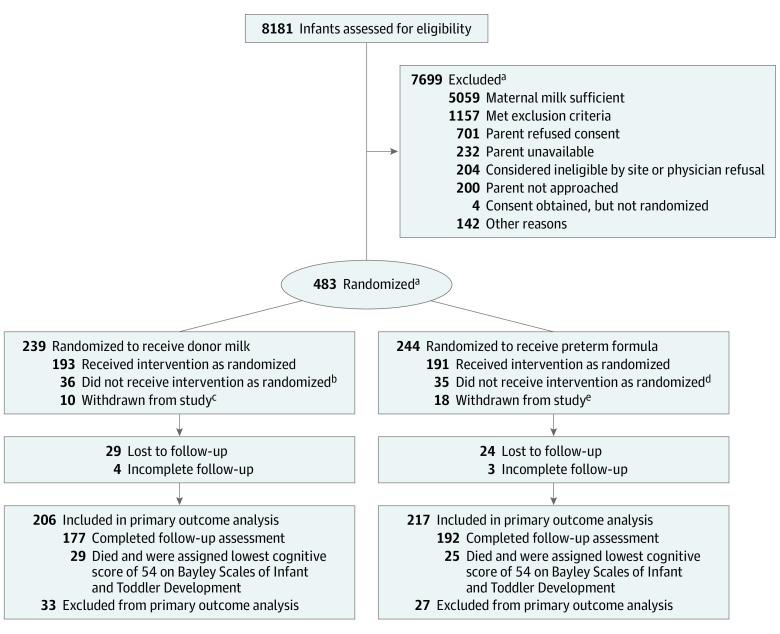
Results: Of 1965 eligible infants, 483 were randomized (239 in the donor milk group and 244 in the preterm formula group); the median gestational age was 26 weeks (IQR, 25-27 weeks), the median birth weight was 840 g (IQR, 676-986 g), and 52% were female. The birthing parent's race was self-reported as Black for 52% (247/478), White for 43% (206/478), and other for 5% (25/478). There were 54 infants who died prior to follow-up; 88% (376/429) of survivors were assessed at 22 to 26 months' corrected age. The adjusted mean BSID cognitive score was 80.7 (SD, 17.4) for the donor milk group vs 81.1 (SD, 16.7) for the preterm formula group (adjusted mean difference, -0.77 [95% CI, -3.93 to 2.39], which was not significant); the adjusted mean BSID language and motor scores also did not differ. Mortality (death prior to follow-up) was 13% (29/231) in the donor milk group vs 11% (25/233) in the preterm formula group (adjusted risk difference, -1% [95% CI, -4% to 2%]). Necrotizing enterocolitis occurred in 4.2% of infants (10/239) in the donor milk group vs 9.0% of infants (22/244) in the preterm formula group (adjusted risk difference, -5% [95% CI, -9% to -2%]). Weight gain was slower in the donor milk group (22.3 g/kg/d [95% CI, 21.3 to 23.3 g/kg/d]) compared with the preterm formula group (24.6 g/kg/d [95% CI, 23.6 to 25.6 g/kg/d]).
Conclusions and relevance: Among extremely preterm neonates fed minimal maternal milk, neurodevelopmental outcomes at 22 to 26 months' corrected age did not differ between infants fed donor milk or preterm formula.
Trial registration: ClinicalTrials.gov Identifier: NCT01534481.
Conflict of interest statement
Figures
Comment in
-
Delivering on the Promise of Human Milk for Extremely Preterm Infants in the NICU.JAMA. 2024 Feb 20;331(7):567-569. doi: 10.1001/jama.2023.26820. JAMA. 2024. PMID: 38289598 No abstract available.
References
-
- Blakely ML, Tyson JE, Lally KP, et al. ; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network . Initial laparotomy versus peritoneal drainage in extremely low birthweight infants with surgical necrotizing enterocolitis or isolated intestinal perforation: a multicenter randomized clinical trial. Ann Surg. 2021;274(4):e370-e380. doi:10.1097/SLA.0000000000005099 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- UG1 HD027853/HD/NICHD NIH HHS/United States
- UG1 HD068284/HD/NICHD NIH HHS/United States
- UG1 HD040492/HD/NICHD NIH HHS/United States
- UG1 HD021364/HD/NICHD NIH HHS/United States
- U01 HD036790/HD/NICHD NIH HHS/United States
- UG1 HD034216/HD/NICHD NIH HHS/United States
- U10 HD021373/HD/NICHD NIH HHS/United States
- UG1 HD068244/HD/NICHD NIH HHS/United States
- UG1 HD027851/HD/NICHD NIH HHS/United States
- UG1 HD027904/HD/NICHD NIH HHS/United States
- UG1 HD068270/HD/NICHD NIH HHS/United States
- UG1 HD068263/HD/NICHD NIH HHS/United States
- UG1 HD021385/HD/NICHD NIH HHS/United States
- U24 HD095254/HD/NICHD NIH HHS/United States
- UG1 HD040689/HD/NICHD NIH HHS/United States
- UG1 HD053109/HD/NICHD NIH HHS/United States
- UG1 HD087226/HD/NICHD NIH HHS/United States
- UG1 HD068278/HD/NICHD NIH HHS/United States
- UG1 HD053089/HD/NICHD NIH HHS/United States
- UG1 HD027856/HD/NICHD NIH HHS/United States
- UG1 HD087229/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
