

Efficacy and Safety of Risankizumab for Active Psoriatic Arthritis: 100-Week Results from the Phase 3 KEEPsAKE 1 Randomized Clinical Trial
- PMID: 38498141
- PMCID: PMC11111619
- DOI: 10.1007/s40744-024-00654-5
Efficacy and Safety of Risankizumab for Active Psoriatic Arthritis: 100-Week Results from the Phase 3 KEEPsAKE 1 Randomized Clinical Trial
Abstract
Introduction: Patients with psoriatic arthritis (PsA) require treatment providing durable long-term efficacy in different disease domains as well as safety. We present 100-week efficacy and safety results of risankizumab in patients with active PsA and previous inadequate response/intolerance to ≥ 1 conventional synthetic disease-modifying antirheumatic drug (csDMARD-IR).
Methods: KEEPsAKE 1 (NCT03675308) is a global phase 3 study, including a 24-week, double-blind, placebo-controlled and ongoing open-label extension periods. Patients were randomized 1:1 to receive risankizumab 150 mg or placebo at baseline and weeks 4 and 16. After week 24, all patients received open-label risankizumab every 12 weeks thereafter. Patients were evaluated through 100 weeks. Endpoints included achieving ≥ 20% reduction in American College of Rheumatology criteria for symptoms of rheumatoid arthritis (ACR20), minimal disease activity (MDA; defined as ≥ 5/7 criteria of low disease activity and extent), and other measures.
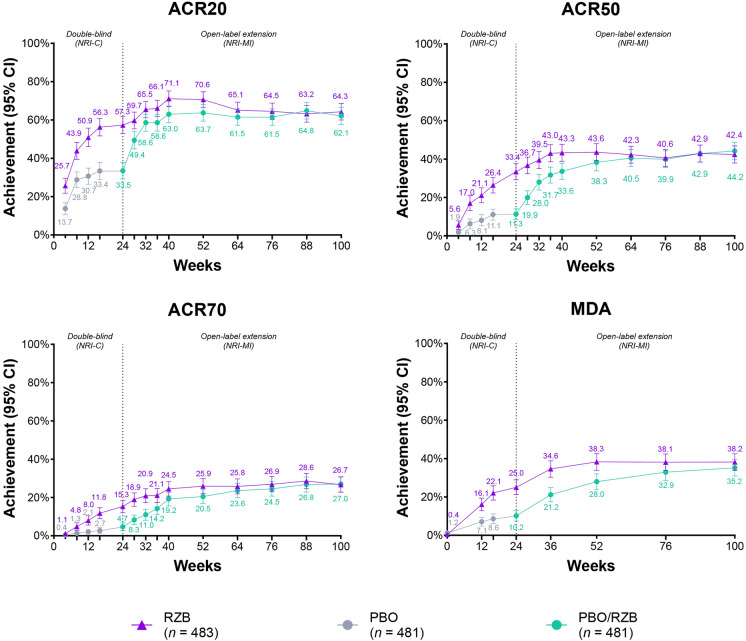
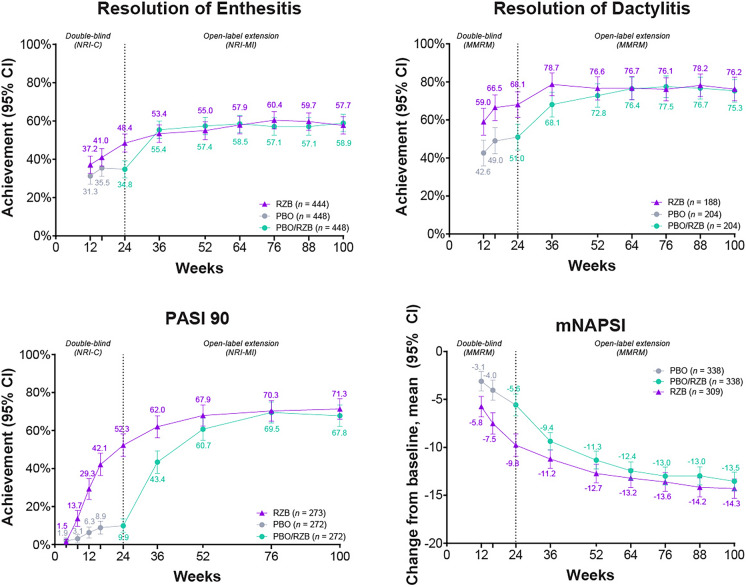
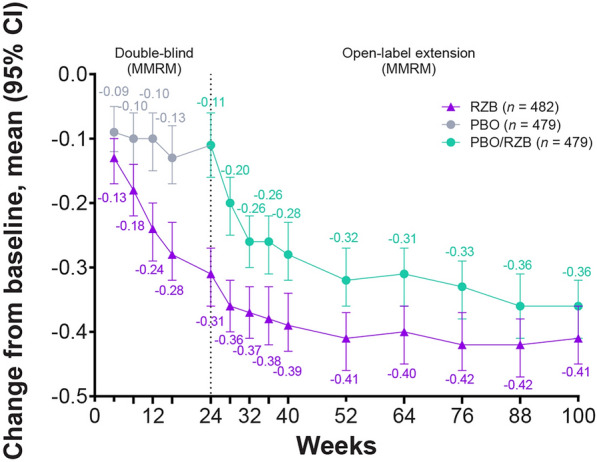
Results: Overall, 828/964 (85.9%) patients completed week 100. For patients receiving continuous risankizumab, 57.3%, 70.6%, and 64.3% achieved ACR20 at weeks 24, 52, and 100, respectively. For the placebo/risankizumab cohort, 33.5% achieved ACR20 at week 24 but increased after switching to active treatment at weeks 52 (63.7%) and 100 (62.1%). In ACR20 responders at week 52, 81.2% of both treatment cohorts maintained response at week 100. MDA was achieved by 25.0%, 38.3%, and 38.2% of the continuous risankizumab cohort at weeks 24, 52, and 100. In the placebo/risankizumab cohort, 10.2% achieved MDA at week 24, increasing at weeks 52 (28.0%) and 100 (35.2%). MDA response was maintained at week 100 in week 52 responders in the continuous risankizumab (75.5%) and placebo/risankizumab cohorts (78.2%). Similar trends were observed for other efficacy measures. Risankizumab was generally well tolerated through 100 weeks.
Conclusions: For patients with active PsA who are csDMARD-IR, risankizumab demonstrated durable long-term efficacy and was generally well tolerated, with a consistent long-term safety profile.
Trial registration: ClinicalTrials.gov identifier, NCT03675308.
Keywords: IL-23; KEEPsAKE 1; Long-term treatment; Psoriatic arthritis; Risankizumab; csDMARD-IR.
Plain language summary
Psoriatic arthritis (PsA) often affects individuals with the skin condition psoriasis. A biologic disease-modifying antirheumatic drug can help control inflammation and regulate the immune system to ease symptoms and slow progression of PsA. The ongoing KEEPsAKE 1 study is evaluating the efficacy and safety of risankizumab in patients with active PsA who previously have not had success with ≥ 1 conventional disease-modifying antirheumatic drug. Patients were initially treated with risankizumab 150 mg (continuous risankizumab group) or inactive drug (inactive drug/risankizumab group). After 24 weeks, all received risankizumab for the rest of the study. At week 100, 64% (continuous risankizumab group) and 62% (inactive drug/risankizumab group) of patients had ≥ 20% improvement in PsA symptoms (measured using American College of Rheumatology [ACR20] criteria). Both groups showed similar percentages at week 52 and improvement from week 24. In patients who achieved ACR20 at week 52, 81% maintained their ACR20 response at week 100. Minimal disease activity was defined as a combination of joint and skin symptoms, affected body surface area, pain, and physical functioning. At week 100, 38% of the continuous risankizumab group and 35% of the inactive drug/risankizumab group achieved minimal disease activity. Percentages were similar at week 52 and higher than week 24 in both groups. In patients who achieved minimal disease activity at week 52, 81% maintained response at week 100. All other measures of treatment responses showed similar patterns from the start of risankizumab through week 100. Risankizumab was considered generally safe by the treating physicians.
© 2024. The Author(s).
Conflict of interest statement
Lars Erik Kristensen has received honoraria or fees for serving as a speaker or consultant from AbbVie, Amgen, Biogen, Bristol Myers Squibb, Gilead, Janssen, Lilly, Merck, Novartis, Pfizer, and UCB. He has also received IIT research grants from Lilly, Novartis, Pfizer, and UCB. Mauro Keiserman has served as a speaker for AbbVie, Bristol Myers Squibb, Celgene, Eli Lilly, Janssen, Novartis, Pfizer, Roche, and UCB; was a consultant for AbbVie, Bristol Myers Squibb, GlaxoSmithKline, MSD, Biogen, Sanofi, and Novartis; and receives grant/research support from AbbVie, Bristol Myers Squibb, GlaxoSmithKline, MSD, Biogen, Sanofi, and Novartis. Kim Papp has received research funds from AbbVie, Aceleryn, Amgen, Arcutis, Bausch Health, Baxalta, Boehringer Ingelheim, Bristol Myers Squibb, Coherus, Dermavant, Forward Pharma, Galderma, Incyte, Janssen, LEO Pharma, Lilly, Novartis, Ortho Dermatologics, Pfizer, Sanofi Genzyme, Sun Pharma, and UCB. He is a consultant for AbbVie, Aceleryn, Amgen, Arcutis, Astellas, Bausch Health, Boehringer Ingelheim, Bristol Myers Squibb, Coherus, Dermavant, Forward Pharma, Galderma, Incyte, Janssen, LEO Pharma, Lilly, Meiji Seika Pharma, Merck, Mitsubishi Tanabe Pharma, Novartis, Pfizer, Sandoz, Sanofi Genzyme, Stiefel, Sun Pharma, Takeda, and UCB. He is a speaker for AbbVie, Amgen, Arcutis, Bausch Health, Boehringer Ingelheim, Bristol Myers Squibb, Dermavant, Incyte, Janssen, LEO Pharma, Lilly, Novartis, Pfizer, Sandoz, Sanofi Genzyme, Sun Pharma, and UCB. He is a committee member for PSOLAR (Psoriasis Longitudinal Assessment and Registry) and PURE (registry of patients with moderate-to-severe chronic plaque psoriasis in Latin America and Canada). Leslie McCasland has received fees for serving on an advisory board from Lilly. Douglas White has received honoraria or fees for serving on advisory boards or as a speaker or consultant from AbbVie. Kyle Carter, Ralph Lippe, Huzefa Photowala, Leonidas Drogaris, Michael Chen, and Byron Padilla are full-time employees of AbbVie, and may hold AbbVie stock or stock options. Ahmed M. Soliman is a full-time employee of AbbVie, may hold AbbVie stock or stock options, and is a coinventor on AbbVie patents. Frank Behrens has received research grants, honoraria, or fees for serving as a consultant or speaker from AbbVie, Amgen, Affibody, Acelyrin, BMS, Boehringer Ingelheim, Chugai, Celltrion, Galapagos, Genzyme, Gilead, GlaxoSmithKline, Janssen, Lilly, Merck, MoonLake, Novartis, Pfizer, Roche, Sandoz and Sanofi.
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
