

Comparing oncologic and surgical outcomes of robotic and laparoscopic pancreatoduodenectomy in patients with pancreatic cancer: a propensity-matched analysis
- PMID: 38498210
- PMCID: PMC11078803
- DOI: 10.1007/s00464-024-10783-1
Comparing oncologic and surgical outcomes of robotic and laparoscopic pancreatoduodenectomy in patients with pancreatic cancer: a propensity-matched analysis
Abstract
Introduction: Minimally invasive Pancreatoduodenectomy (MIPD), or the Whipple procedure, is increasingly utilized. No study has compared laparoscopic (LPD) and robotic (RPD) approaches, and the impact of the learning curve on oncologic, technical, and post-operative outcomes remains relatively understudied.
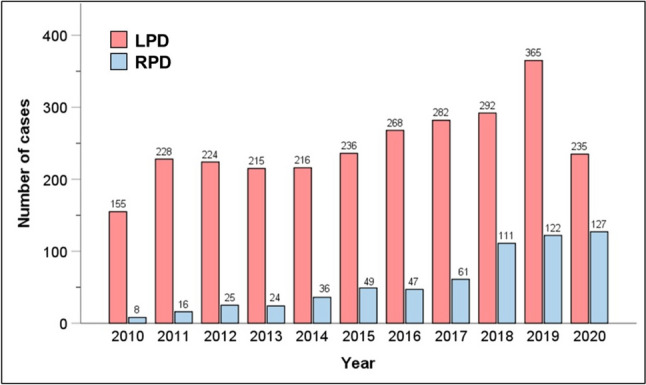
Methods: The National Cancer Database was queried for patients undergoing LPD or RPD from 2010 to 2020 with a diagnosis of pancreatic cancer. Outcomes were compared between approaches using propensity-score matching (PSM); the impact of annual center-level volume of MIPD was also assessed by dividing volume into quartiles.
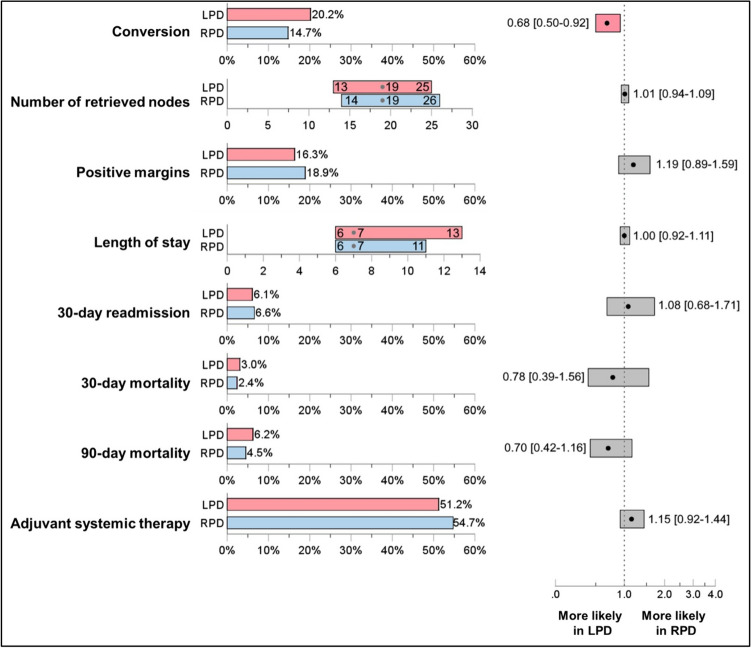
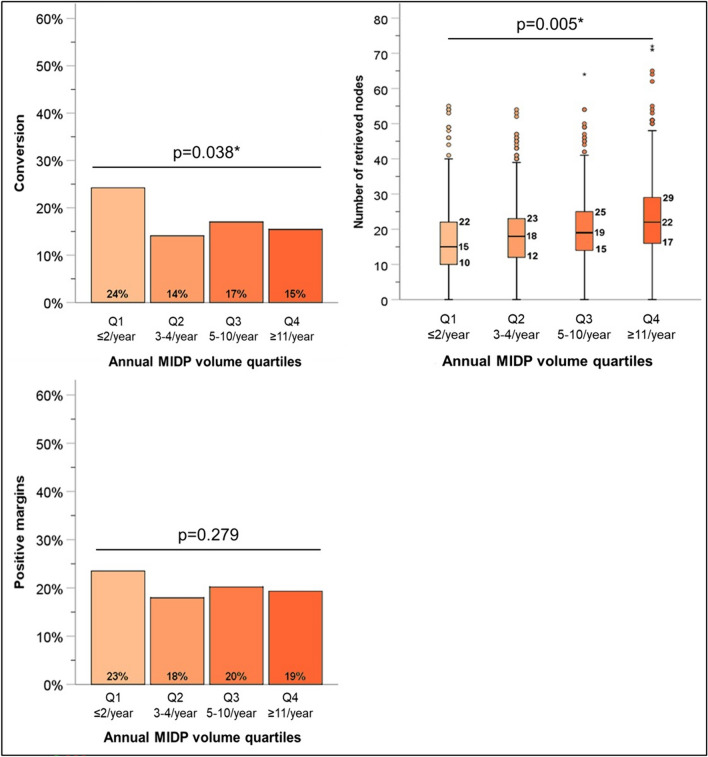
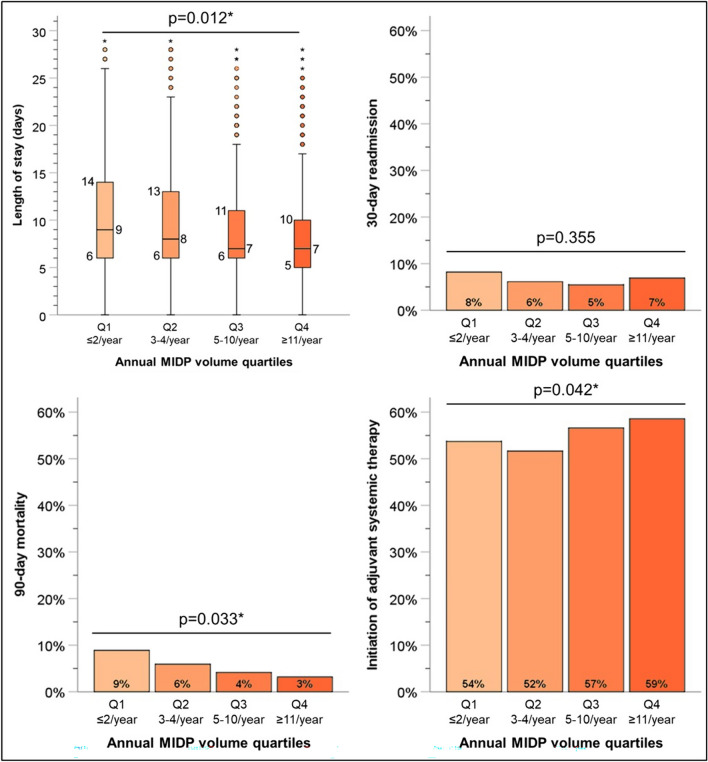
Results: A total of 3,342 patients were included. Most (n = 2,716, 81.3%) underwent LPD versus RPD (n = 626, 18.7%). There was a high rate (20.2%, n = 719) of positive margins. Mean length-of-stay (LOS) was 10.4 ± 8.9 days. Thirty-day mortality was 2.8% (n = 92) and ninety-day mortality was 5.7% (n = 189). PSM matched 625 pairs of patients receiving LPD or RPD. After PSM, there was no differences between groups based on age, sex, race, CCI, T-stage, neoadjuvant chemo/radiotherapy, or type of PD. After PSM, there was a higher rate of conversion to open (HR = 0.68, 95%CI = 0.50-0.92)., but there was no difference in LOS (HR = 1.00, 95%CI = 0.92-1.11), 30-day readmission (HR = 1.08, 95% CI = 0.68-1.71), 30-day (HR = 0.78, 95% CI = 0.39-1.56) or 90-day mortality (HR = 0.70, 95% CI = 0.42-1.16), ability to receive adjuvant therapy (HR = 1.15, 95% CI = 0.92-1.44), nodal harvest (HR = 1.01, 95%CI = 0.94-1.09) or positive margins (HR = 1.19, 95% CI = 0.89-1.59). Centers in lower quartiles of annual volume of MIPD demonstrated reduced nodal harvest (p = 0.005) and a higher rate of conversion to open (p = 0.038). Higher-volume centers had a shorter LOS (p = 0.012), higher rate of initiation of adjuvant therapy (p = 0.042), and, most strikingly, a reduction in 90-day mortality (p = 0.033).
Conclusion: LPD and RPD have similar surgical and oncologic outcomes, with a lower rate of conversion to open in the robotic cohort. The robotic technique does not appear to eliminate the "learning curve", with higher volume centers demonstrating improved outcomes, especially seen at minimum annual volume of 5 cases.
Keywords: Laparoscopic surgery; Minimally invasive surgery; Pancreatic ductal adenocarcinoma; Pancreatoduodenectomy; Robotic surgery.
© 2024. The Author(s).
Conflict of interest statement
Drs. Chase J. Wehrle, Jenny H. Chang, Abby R. Gross, Kimberly Woo, Robert Naples, Kathryn A. Stackhouse, Fadi Dahdaleh, Toms Augustin, Daniel Joyce, Robert Simon, R. Matthew Walsh and Samer A. Naffouje have no conflicts of interest or financial ties to disclose.
Figures
Similar articles
-
Comparing oncologic and surgical outcomes of robotic and laparoscopic distal pancreatectomy: a propensity-matched analysis.Surg Endosc. 2024 Oct;38(10):5678-5685. doi: 10.1007/s00464-024-11147-5. Epub 2024 Aug 12. Surg Endosc. 2024. PMID: 39134718 Free PMC article.
-
Comparing Short-term and Oncologic Outcomes of Minimally Invasive Versus Open Pancreaticoduodenectomy Across Low and High Volume Centers.Ann Surg. 2019 Dec;270(6):1147-1155. doi: 10.1097/SLA.0000000000002810. Ann Surg. 2019. PMID: 29771723
-
Robotic-assisted versus laparoscopic pancreaticoduodenectomy: oncological outcomes.Surg Endosc. 2018 Jun;32(6):2907-2913. doi: 10.1007/s00464-017-6002-2. Epub 2017 Dec 26. Surg Endosc. 2018. PMID: 29280014
-
Postoperative complications and surgical outcomes of robotic versus laparoscopic pancreaticoduodenectomy: a meta-analysis of propensity-score-matched studies.Int J Surg. 2025 Feb 1;111(2):2257-2272. doi: 10.1097/JS9.0000000000002196. Int J Surg. 2025. PMID: 39715160
-
State of the art of robotic pancreatoduodenectomy.Updates Surg. 2021 Jun;73(3):873-880. doi: 10.1007/s13304-021-01058-8. Epub 2021 May 20. Updates Surg. 2021. PMID: 34014497 Free PMC article. Review.
Cited by
-
Robotic pancreatoduodenectomy provides better short-term outcomes as compared to its laparoscopic counterpart: a meta-analysis.Front Oncol. 2025 Jun 18;15:1568957. doi: 10.3389/fonc.2025.1568957. eCollection 2025. Front Oncol. 2025. PMID: 40606993 Free PMC article.
-
Effects of Minimally Invasive Versus Open Pancreatoduodenectomy on Short-Term Surgical Outcomes and Postoperative Nutritional and Immunological Statuses: A Single-Institution Propensity Score-Matched Study.Ann Surg Open. 2024 Aug 30;5(3):e487. doi: 10.1097/AS9.0000000000000487. eCollection 2024 Sep. Ann Surg Open. 2024. PMID: 39310352 Free PMC article.
-
Robotic vs laparoscopic approaches of pancreatic resection: a systematic review and meta-analysis.J Robot Surg. 2025 Jun 16;19(1):295. doi: 10.1007/s11701-025-02446-7. J Robot Surg. 2025. PMID: 40522553 Review.
-
Comparing the operative, oncological, post-operative outcomes and complications of robotic and laparoscopic pancreaticoduodenectomy for the treatment of pancreatic and periampullary cancers: a systematic review and meta-analysis with subgroup analysis.J Robot Surg. 2025 Mar 5;19(1):97. doi: 10.1007/s11701-025-02239-y. J Robot Surg. 2025. PMID: 40042699
-
Robotic versus laparoscopic pancreaticoduodenectomy for pancreatic and periampullary tumors: a meta-analysis.Front Oncol. 2024 Nov 19;14:1486504. doi: 10.3389/fonc.2024.1486504. eCollection 2024. Front Oncol. 2024. PMID: 39629002 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
