

Education to improve timeliness of shingles diagnosis in primary care: a cluster randomised study within a trial with nested qualitative study
- PMID: 38499295
- PMCID: PMC11349368
- DOI: 10.3399/BJGP.2023.0477
Education to improve timeliness of shingles diagnosis in primary care: a cluster randomised study within a trial with nested qualitative study
Abstract
Background: Herpes zoster (shingles) is normally diagnosed clinically. Timely diagnosis is important so that antiviral treatment can be started soon after rash onset.
Aim: To assess whether a practice-level educational intervention, aimed at non-clinical patient-facing staff, improves the timely assessment of patients with shingles.
Design and setting: This was a cluster randomised study within a trial (SWAT) with nested qualitative study in general practices in England.
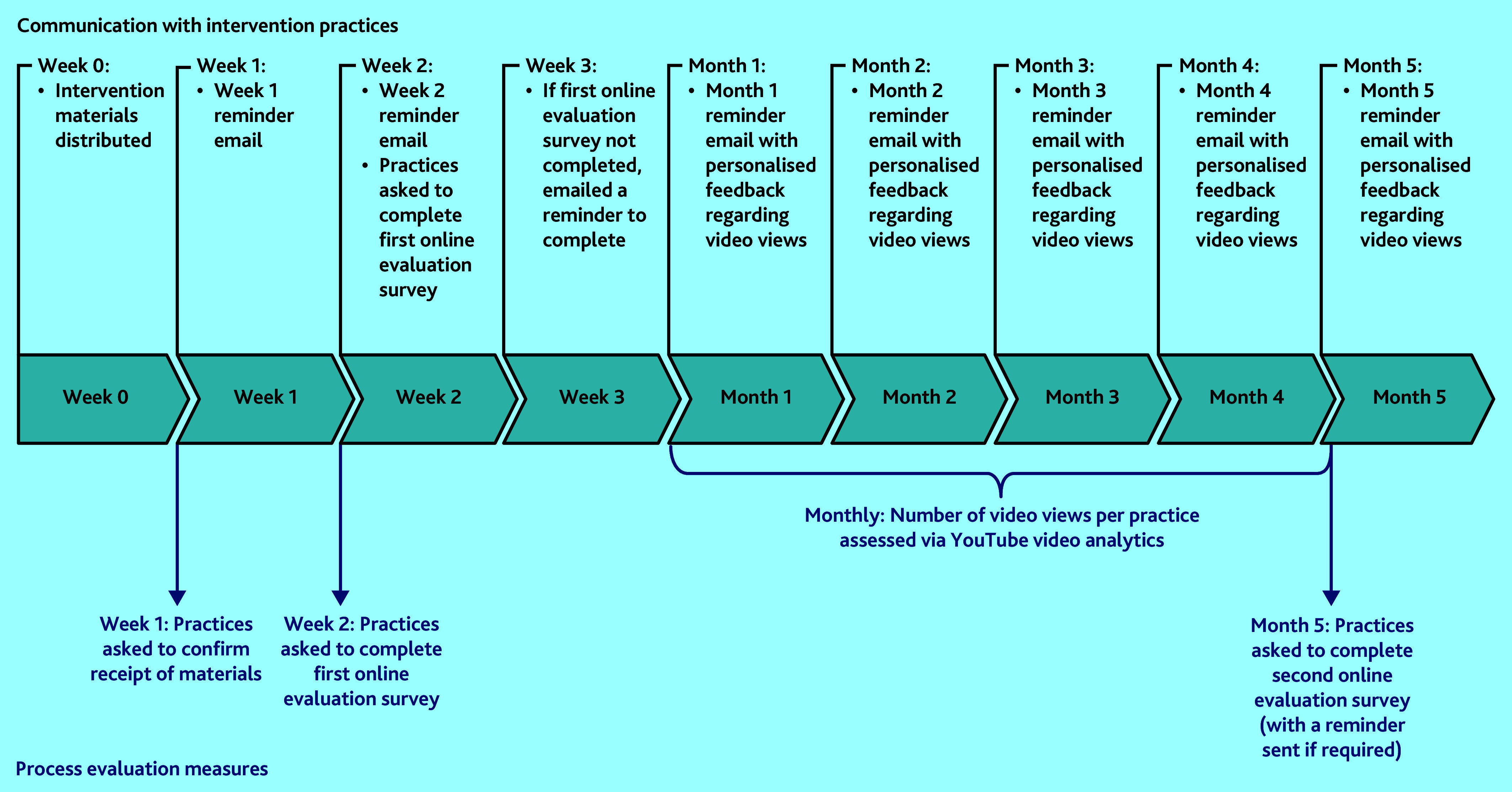
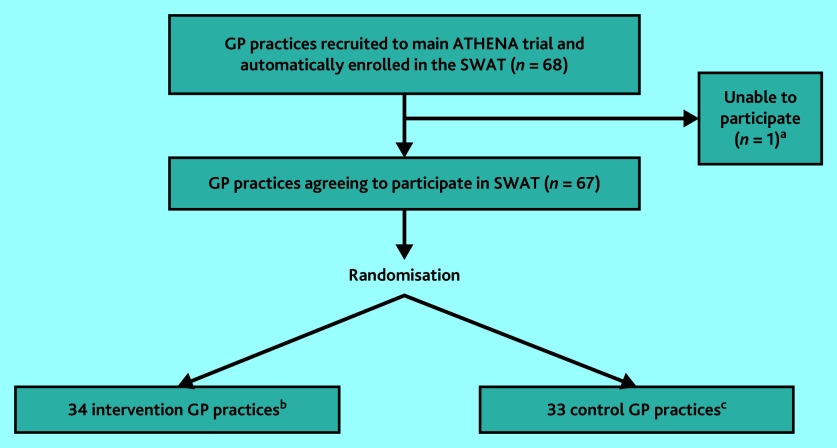
Method: Practices were cluster randomised 1:1, stratified by centre and minimised by practice list size and Index of Multiple Deprivation score. Intervention practices were sent educational materials, highlighting the common presenting features of shingles and what action to take if suspected. The primary and secondary outcomes were the mean proportion of patients per practice seen within 72 and 144 h of rash onset, respectively. Comparison between groups was conducted using linear regression, adjusting for randomisation variables. Semi-structured interviews with practice staff in intervention practices explored views and opinions about the intervention.
Results: In total, 67 practices were enrolled; 34 randomised to the intervention and 33 to the control. The mean difference in proportion of patients seen within 72 and 144 h was -0.132 (95% confidence interval [CI] = -0.308 to 0.043) and -0.039 (95% CI = -0.158 to 0.080), respectively. In intervention practices, 90.9% reported distributing the educational materials; however, engagement with these was suboptimal. Twelve participants were interviewed, and the poster component of the intervention was said to be easiest to implement.
Conclusion: Our educational intervention did not improve the timely assessment of patients with shingles. This may be the result of poor intervention engagement.
Keywords: diagnosis; general practice; herpes zoster; interprofessional education.
© The Authors.
Conflict of interest statement
The authors have declared no competing interests.
Figures
Similar articles
-
'Everyone has heard of it, but no one knows what it is': a qualitative study of patient understandings and experiences of herpes zoster.Br J Gen Pract. 2025 Jan 30;75(751):e137-e142. doi: 10.3399/BJGP.2024.0025. Print 2025 Feb. Br J Gen Pract. 2025. PMID: 39084872 Free PMC article.
-
Lower urinary tract symptoms in men: the TRIUMPH cluster RCT.Health Technol Assess. 2024 Mar;28(13):1-162. doi: 10.3310/GVBC3182. Health Technol Assess. 2024. PMID: 38512051 Free PMC article. Clinical Trial.
-
Structured, intensive education maximising engagement, motivation and long-term change for children and young people with diabetes: a cluster randomised controlled trial with integral process and economic evaluation - the CASCADE study.Health Technol Assess. 2014 Mar;18(20):1-202. doi: 10.3310/hta18200. Health Technol Assess. 2014. PMID: 24690402 Free PMC article. Clinical Trial.
-
Current experience and future potential of facilitating access to digital NHS primary care services in England: the Di-Facto mixed-methods study.Health Soc Care Deliv Res. 2024 Sep;12(32):1-197. doi: 10.3310/JKYT5803. Health Soc Care Deliv Res. 2024. PMID: 39324475 Review.
-
[Reactivation of herpes zoster infection by varicella-zoster virus].Med Pregl. 1999 Mar-May;52(3-5):125-8. Med Pregl. 1999. PMID: 10518396 Review. Croatian.
References
-
- National Institute for Health and Care Excellence (NICE) Shingles. London: NICE; 2024. https://cks.nice.org.uk/topics/shingles (accessed 17 Jul 2024).
-
- Saguil A, Kane S, Mercado M, Lauters R. herpes zoster and postherpetic neuralgia: prevention and management. Am Fam Physician. 2017;96(10):656–663. - PubMed
-
- Werner RN, Nikkels AF, Marinović B, et al. European consensus-based (S2k) Guideline on the Management of Herpes Zoster − guided by the European Dermatology Forum (EDF) in cooperation with the European Academy of Dermatology and Venereology (EADV), Part 2: treatment. J Eur Acad Dermatol Venereol. 2017;31(1):20–29. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical