

Presentation, Management, and Outcomes of Thoracic, Thoracolumbar, and Lumbar Spine Trauma in East Africa: A Cohort Study
- PMID: 38499345
- PMCID: PMC11287825
- DOI: 10.14444/8575
Presentation, Management, and Outcomes of Thoracic, Thoracolumbar, and Lumbar Spine Trauma in East Africa: A Cohort Study
Abstract
Background: Trauma to the thoracic, thoracolumbar (TL), and lumbar spine is common and can cause disability and neurological deficits. Using a cohort of patients suffering from thoracic, TL, and lumbar spine trauma in a tertiary hospital in East Africa, the current study sought to: (1) describe demographics and operative treatment patterns, (2) assess neurologic outcomes, and (3) report predictors associated with undergoing surgery, neurologic improvement, and mortality.
Methods: A retrospective cohort study of patient records from September 2016 to December 2020 was conducted at a prominent East Africa referral center. The study collected data on demographics, injury, and operative characteristics. Surgical indications were assessed using the AO (Arbeitsgemeinschaft für Osteosynthesefragen) TL fracture classification system and neurological function. Logistic regression analysis identified predictors for operative treatment, neurologic improvement, and mortality.
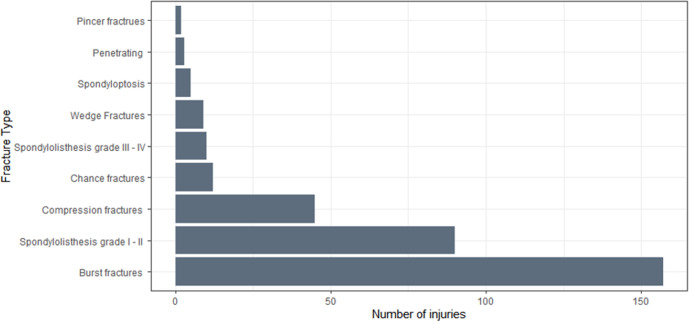
Results: The study showed that 64.9% of the 257 TL spine trauma patients underwent surgery with a median postadmission day of 17.0. The mortality rate was 1.2%. Road traffic accidents caused 43.6% of the injuries. The most common fracture pattern was AO Type A fractures (78.6%). Laminectomy and posterolateral fusion were performed in 97.6% of the surgical cases. Patients without neurological deficits (OR: 0.27, 95% CI: 0.13-0.54, P < 0.001) and those with longer delays from injury to admission were less likely to have surgery (OR: 0.95, 95% CI: 0.92-0.99, P = 0.007). The neurologic improvement rate was 11.1%. Univariate analysis showed a significant association between surgery and neurologic improvement (OR: 3.83, 95% CI: 1.27-16.61, P < 0.001). However, this finding was lost in multivariate regression.
Conclusions: This study highlights various themes surrounding the management of TL spine trauma in a low-resource environment, including lower surgery rates, delays from admission to surgery, safe surgery with low mortality, and the potential for surgery to lead to neurologic improvement.
Clinical relevance: Despite challenges such as surgical delays and limited resources in East Africa, there is potential for surgical intervention to improve neurologic outcomes in thoracic, TL, and lumbar spine trauma patients.
Keywords: LMICs; Tanzania; spine trauma; thoracolumbar; traumatic spinal cord injury.
This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources