

Hematopoietic stem cells with granulo-monocytic differentiation state overcome venetoclax sensitivity in patients with myelodysplastic syndromes
- PMID: 38499526
- PMCID: PMC10948794
- DOI: 10.1038/s41467-024-46424-3
Hematopoietic stem cells with granulo-monocytic differentiation state overcome venetoclax sensitivity in patients with myelodysplastic syndromes
Abstract
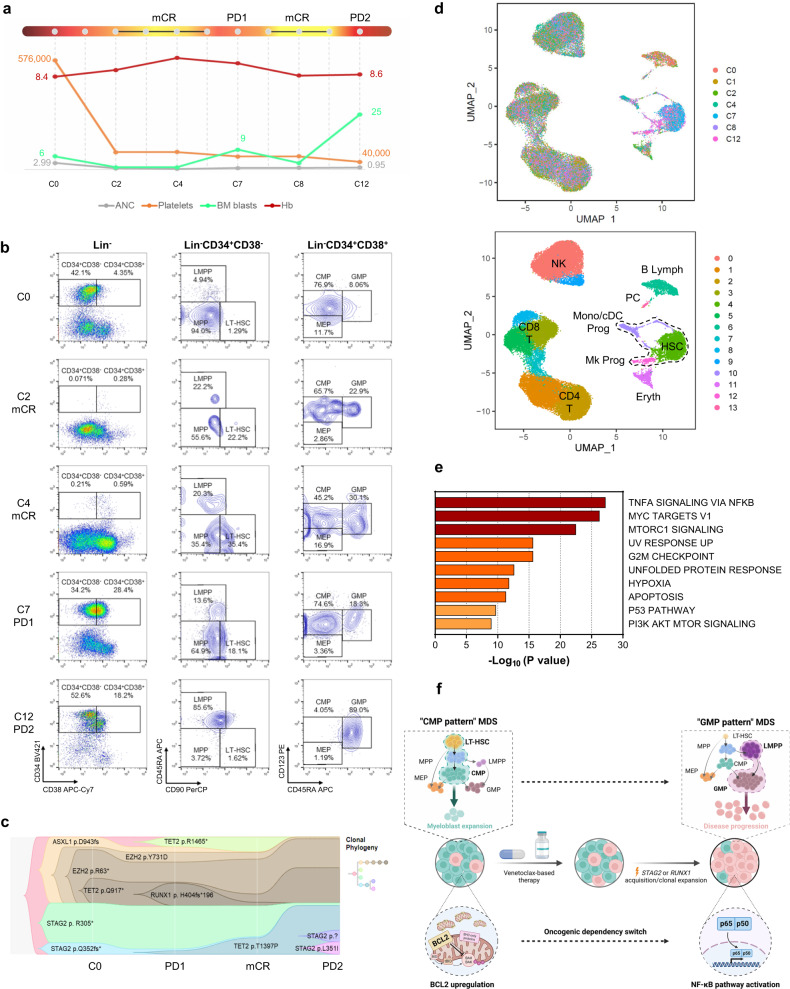
The molecular mechanisms of venetoclax-based therapy failure in patients with acute myeloid leukemia were recently clarified, but the mechanisms by which patients with myelodysplastic syndromes (MDS) acquire secondary resistance to venetoclax after an initial response remain to be elucidated. Here, we show an expansion of MDS hematopoietic stem cells (HSCs) with a granulo-monocytic-biased transcriptional differentiation state in MDS patients who initially responded to venetoclax but eventually relapsed. While MDS HSCs in an undifferentiated cellular state are sensitive to venetoclax treatment, differentiation towards a granulo-monocytic-biased transcriptional state, through the acquisition or expansion of clones with STAG2 or RUNX1 mutations, affects HSCs' survival dependence from BCL2-mediated anti-apoptotic pathways to TNFα-induced pro-survival NF-κB signaling and drives resistance to venetoclax-mediated cytotoxicity. Our findings reveal how hematopoietic stem and progenitor cell (HSPC) can eventually overcome therapy-induced depletion and underscore the importance of using close molecular monitoring to prevent HSPC hierarchical change in MDS patients enrolled in clinical trials of venetoclax.
© 2024. The Author(s).
Conflict of interest statement
G.G.-M. reports clinical funding from AbbVie and Amgen. All other authors report no competing interests relative to this work.
Figures
References
-
- Bazinet A, et al. Azacitidine plus venetoclax in patients with high-risk myelodysplastic syndromes or chronic myelomonocytic leukaemia: phase 1 results of a single-centre, dose-escalation, dose-expansion, phase 1-2 study. Lancet Haematol. 2022;9:e756–e765. doi: 10.1016/S2352-3026(22)00216-2. - DOI - PubMed
-
- Nechiporuk T, et al. The TP53 apoptotic network is a primary mediator of resistance to BCL2 inhibition in AML cells. Cancer Discov. 2019;9:910–925. doi: 10.1158/2159-8290.CD-19-0125. - DOI - PMC - PubMed
-
- Pei S, et al. Monocytic subclones confer resistance to venetoclax-based therapy in patients with acute myeloid leukemia. Cancer Discov. 2020;10:536–551. doi: 10.1158/2159-8290.CD-19-0710. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
