

Dynamic associations between glucose and ecological momentary cognition in Type 1 Diabetes
- PMID: 38499605
- PMCID: PMC10948782
- DOI: 10.1038/s41746-024-01036-5
Dynamic associations between glucose and ecological momentary cognition in Type 1 Diabetes
Abstract
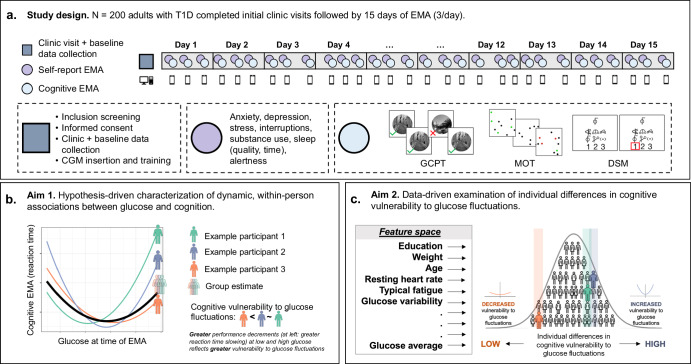
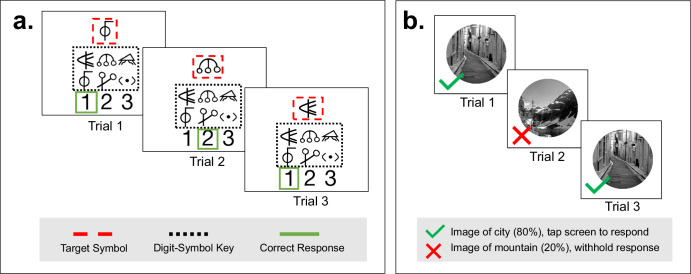
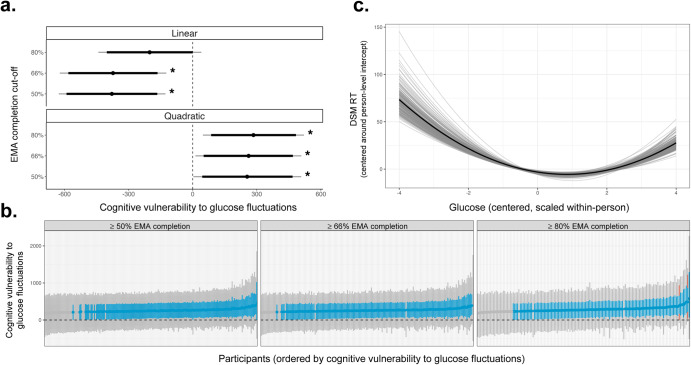
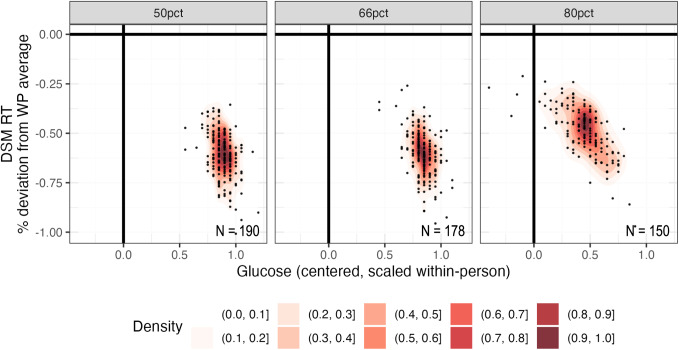
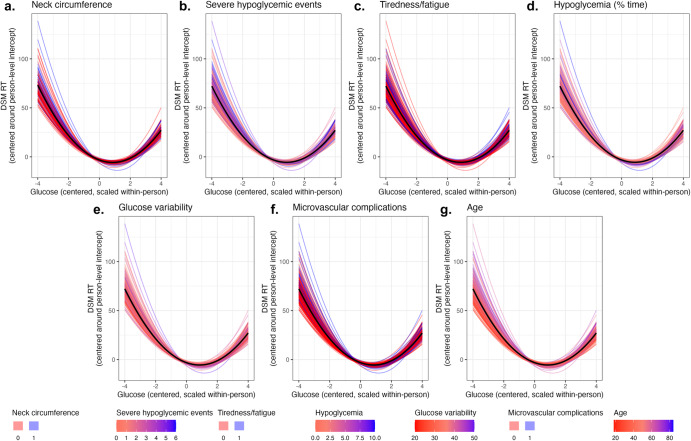
Type 1 diabetes (T1D) is a chronic condition characterized by glucose fluctuations. Laboratory studies suggest that cognition is reduced when glucose is very low (hypoglycemia) and very high (hyperglycemia). Until recently, technological limitations prevented researchers from understanding how naturally-occurring glucose fluctuations impact cognitive fluctuations. This study leveraged advances in continuous glucose monitoring (CGM) and cognitive ecological momentary assessment (EMA) to characterize dynamic, within-person associations between glucose and cognition in naturalistic environments. Using CGM and EMA, we obtained intensive longitudinal measurements of glucose and cognition (processing speed, sustained attention) in 200 adults with T1D. First, we used hierarchical Bayesian modeling to estimate dynamic, within-person associations between glucose and cognition. Consistent with laboratory studies, we hypothesized that cognitive performance would be reduced at low and high glucose, reflecting cognitive vulnerability to glucose fluctuations. Second, we used data-driven lasso regression to identify clinical characteristics that predicted individual differences in cognitive vulnerability to glucose fluctuations. Large glucose fluctuations were associated with slower and less accurate processing speed, although slight glucose elevations (relative to person-level means) were associated with faster processing speed. Glucose fluctuations were not related to sustained attention. Seven clinical characteristics predicted individual differences in cognitive vulnerability to glucose fluctuations: age, time in hypoglycemia, lifetime severe hypoglycemic events, microvascular complications, glucose variability, fatigue, and neck circumference. Results establish the impact of glucose on processing speed in naturalistic environments, suggest that minimizing glucose fluctuations is important for optimizing processing speed, and identify several clinical characteristics that may exacerbate cognitive vulnerability to glucose fluctuations.
© 2024. The Author(s).
Conflict of interest statement
LG is on the Board of Directors of the Many Brains Project, a 501c3 nonprofit organization that disseminates cognitive tests. NC is a paid consultant for Adaptelligence, LLC. ZWH and MRF have received consulting fees from Blueprint Health. SS has received consulting fees from Aphelion Capital. RSW has participated in multicenter clinical trials through her institution sponsored by Eli Lilly Novo Nordisk, Insulet, Tandem, Amgen, MannKind and Diasome and has used devices donated by DexCom in research studies. YCK has had product support from Dexcom Inc. and Tandem Inc., is on an advisory board for Novo Nordisk, USA, and has participated in multicenter clinical trials through his institution funded by Dexcom, Tandem, Medtronic and Mannkind. HVD is a paid consultant for Jazz Pharmaceuticals. The authors declare no other competing interests.
Figures
References
-
- Ozougwu JC, Obimba KC, Belonwu CD, Unakalamba CB. The pathogenesis and pathophysiology of type 1 and type 2 diabetes mellitus. J. Physiol. Pathophysiol. 2013;4:46–57. doi: 10.5897/JPAP2013.0001. - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
