

Imaging features of intra-abdominal and intra-pelvic causes of hirsutism
- PMID: 38499827
- PMCID: PMC11213803
- DOI: 10.1007/s00261-024-04189-9
Imaging features of intra-abdominal and intra-pelvic causes of hirsutism
Abstract
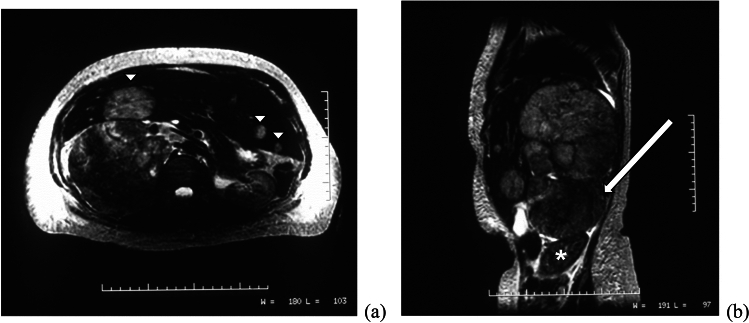
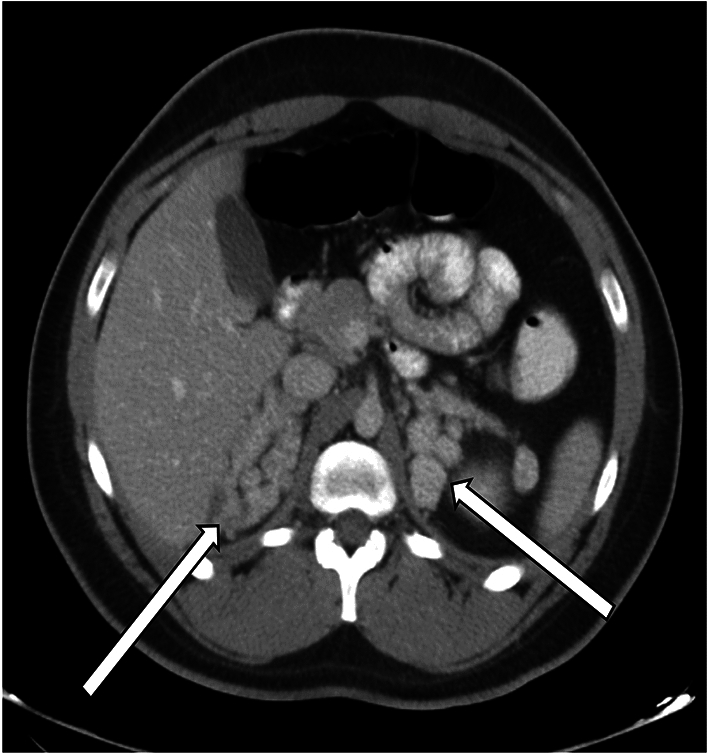
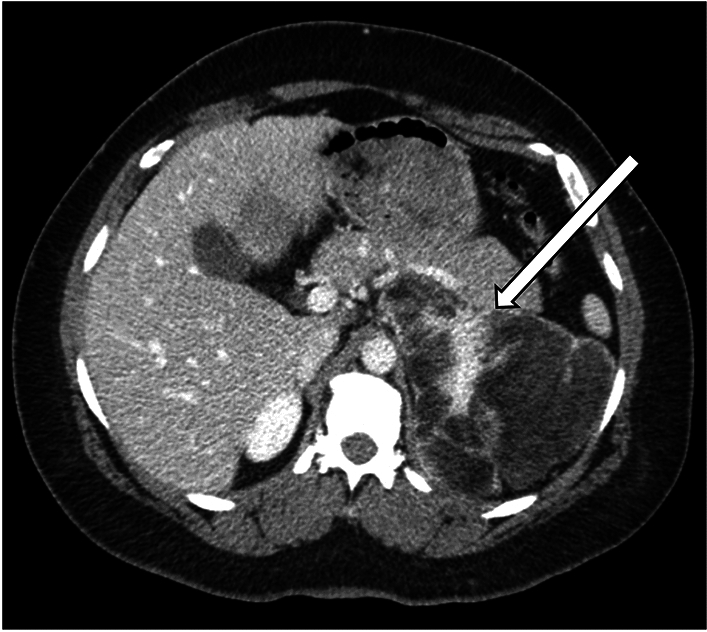
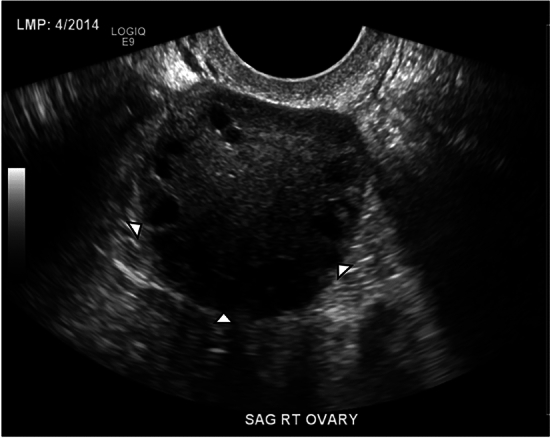
Hirsutism is a relatively common disorder which affects approximately 5% to 15% of women. It is defined by excessive growth of terminal hair in women, which primarily affects areas dependent on androgens, such as the face, abdomen, buttocks, and thighs. Hirsutism can be caused by a variety of etiologies, which are most often not lifethreatening. However, in some cases, hirsutism can be an indicator of more serious underlying pathology, such as a neoplasm, which may require further elucidation with imaging. Within the abdomen and pelvis, adrenal and ovarian pathologies are the primary consideration. The goal of this manuscript is to review the etiologies and imaging features of various intra-abdominal and intra-pelvic causes of hirsutism.
Keywords: Adrenal; Hirsutism; Hyperandrogenism; Imaging features; Ovarian.
© 2024. The Author(s).
Figures




Similar articles
-
Hirsutism and virilism in women.Spec Top Endocrinol Metab. 1984;6:55-93. Spec Top Endocrinol Metab. 1984. PMID: 6084314 Review.
-
[Hyperandrogenism in women].Presse Med. 2013 Nov;42(11):1487-99. doi: 10.1016/j.lpm.2013.07.016. Epub 2013 Nov 1. Presse Med. 2013. PMID: 24184282 Review. French.
-
[Dehydroepiandrosterone sulfate in the differential diagnosis of adrenal and ovarian dysfunction in women with hirsutism and anovulation].Cesk Gynekol. 1986 Apr;51(3):160-6. Cesk Gynekol. 1986. PMID: 2941167 Czech. No abstract available.
-
Dexamethasone-suppression adrenal scintigraphy in hyperandrogenism: concise communication.J Nucl Med. 1981 Jan;22(1):12-7. J Nucl Med. 1981. PMID: 7452350
-
[Hirsutism, what can be done?].Schweiz Rundsch Med Prax. 1992 Apr 14;81(16):511-8. Schweiz Rundsch Med Prax. 1992. PMID: 1574670 Review. French.
References
-
- Matheson E, Bain J. Hirsutism in Women. Am Fam Physician. 2019; 100(3): 168–175. https://www.aafp.org/pubs/afp/issues/2019/0801/p168.html - PubMed
-
- Hafsi W, Badri T. Hirsutism. StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. https://www.ncbi.nlm.nih.gov/books/NBK470417/
-
- Franks S. The investigation and management of hirsutism. Journal of Family Planning and Reproductive Health Care. 2012; 38: 182–186. https://srh.bmj.com/content/38/3/182 - PubMed
-
- Winterson E, Eyster K, Hansen KA. An Uncommon Etiology For A Common Problem: Hirsutism. S D Med. 2011; 64(5): 161–3, 165. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
