

Increased functional connectivity between default mode network and visual network potentially correlates with duration of residual dizziness in patients with benign paroxysmal positional vertigo
- PMID: 38500812
- PMCID: PMC10944895
- DOI: 10.3389/fneur.2024.1363869
Increased functional connectivity between default mode network and visual network potentially correlates with duration of residual dizziness in patients with benign paroxysmal positional vertigo
Abstract
Objective: To assess changes in static and dynamic functional network connectivity (sFNC and dFNC) and explore their correlations with clinical features in benign paroxysmal positional vertigo (BPPV) patients with residual dizziness (RD) after successful canalith repositioning maneuvers (CRM) using resting-state fMRI.
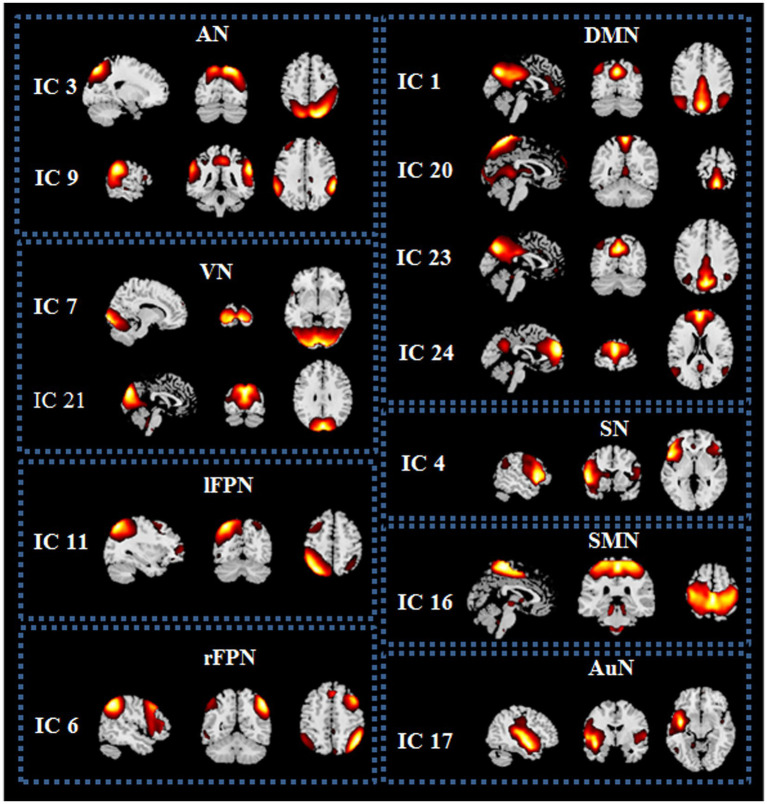
Methods: We studied resting-state fMRI data from 39 BPPV patients with RD compared to 38 BPPV patients without RD after successful CRM. Independent component analysis and methods of sliding window and k-means clustering were adopted to investigate the changes in dFNC and sFNC between the two groups. Additionally, temporal features and meta-states were compared between the two groups. Furthermore, the associations between fMRI results and clinical characteristics were analyzed using Pearson's partial correlation analysis.
Results: Compared with BPPV patients without RD, patients with RD had longer duration of BPPV and higher scores of dizziness handicap inventory (DHI) before successful CRM. BPPV patients with RD displayed no obvious abnormal sFNC compared to patients without RD. In the dFNC analysis, patients with RD showed increased FNC between default mode network (DMN) and visual network (VN) in state 4, the FNC between DMN and VN was positively correlated with the duration of RD. Furthermore, we found increased mean dwell time (MDT) and fractional windows (FW) in state 1 but decreased MDT and FW in state 3 in BPPV patients with RD. The FW of state 1 was positively correlated with DHI score before CRM, the MDT and FW of state 3 were negatively correlated with the duration of BPPV before CRM in patients with RD. Additionally, compared with patients without RD, patients with RD showed decreased number of states and state span.
Conclusion: The occurrence of RD might be associated with increased FNC between DMN and VN, and the increased FNC between DMN and VN might potentially correlate with the duration of RD symptoms. In addition, we found BPPV patients with RD showed altered global meta-states and temporal features. These findings are helpful for us to better understand the underlying neural mechanisms of RD and potentially contribute to intervention development for BPPV patients with RD.
Keywords: benign paroxysmal positional vertigo; dynamic functional network connectivity; independent component analysis; residual dizziness; resting-state fMRI; static functional network connectivity.
Copyright © 2024 Chen, Cai, Xiao, Wei, Liu, Lin, Liu, Liu and Rong.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





Similar articles
-
Altered Hippocampal Subfields Functional Connectivity in Benign Paroxysmal Positional Vertigo Patients With Residual Dizziness: A Resting-State fMRI Study.CNS Neurosci Ther. 2024 Dec;30(12):e70175. doi: 10.1111/cns.70175. CNS Neurosci Ther. 2024. PMID: 39690894 Free PMC article.
-
Altered parietal operculum cortex 2 functional connectivity in benign paroxysmal positional vertigo patients with residual dizziness: A resting-state fMRI study.CNS Neurosci Ther. 2024 Feb;30(2):e14570. doi: 10.1111/cns.14570. CNS Neurosci Ther. 2024. PMID: 38421104 Free PMC article.
-
Assessment of residual dizziness after successful canalith repositioning maneuvre in benign paroxysmal positional vertigo patients: a questionnaire-based study.Eur Arch Otorhinolaryngol. 2023 Jan;280(1):137-141. doi: 10.1007/s00405-022-07474-9. Epub 2022 Jun 21. Eur Arch Otorhinolaryngol. 2023. PMID: 35727415
-
Poor Treatment Outcomes Following Repositioning Maneuvers in Younger and Older Adults With Benign Paroxysmal Positional Vertigo: A Systematic Review and Meta-analysis.J Am Med Dir Assoc. 2019 Feb;20(2):224.e1-224.e23. doi: 10.1016/j.jamda.2018.11.019. J Am Med Dir Assoc. 2019. PMID: 30691621
-
Residual dizziness after BPPV management: exploring pathophysiology and treatment beyond canalith repositioning maneuvers.Front Neurol. 2024 May 24;15:1382196. doi: 10.3389/fneur.2024.1382196. eCollection 2024. Front Neurol. 2024. PMID: 38854956 Free PMC article. Review.
Cited by
-
Altered Hippocampal Subfields Functional Connectivity in Benign Paroxysmal Positional Vertigo Patients With Residual Dizziness: A Resting-State fMRI Study.CNS Neurosci Ther. 2024 Dec;30(12):e70175. doi: 10.1111/cns.70175. CNS Neurosci Ther. 2024. PMID: 39690894 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous