

Trends in Lower Extremity Artery Disease Repair Incidence, Comorbidity, and Mortality: A Danish Nationwide Cohort Study, 1996-2018
- PMID: 38501043
- PMCID: PMC10946405
- DOI: 10.2147/VHRM.S427211
Trends in Lower Extremity Artery Disease Repair Incidence, Comorbidity, and Mortality: A Danish Nationwide Cohort Study, 1996-2018
Abstract
Background: The prevalence of occlusive lower extremity artery disease (LEAD) is rising worldwide while European epidemiology data are scarce. We report incidence and mortality of LEAD repair in Denmark from 1996 through 2018, stratified on open aorto-iliac, open peripheral, and endovascular repair.
Methods: A nationwide cohort study of prospective data from population-based Danish registers covering 1996 to 2018. Comorbidity was assessed by Charlson's Comorbidity Index (CCI). Incidence rate (IR) ratios and mortality rate ratios (MRR) were estimated by multivariable Poisson and Cox regression, respectively.
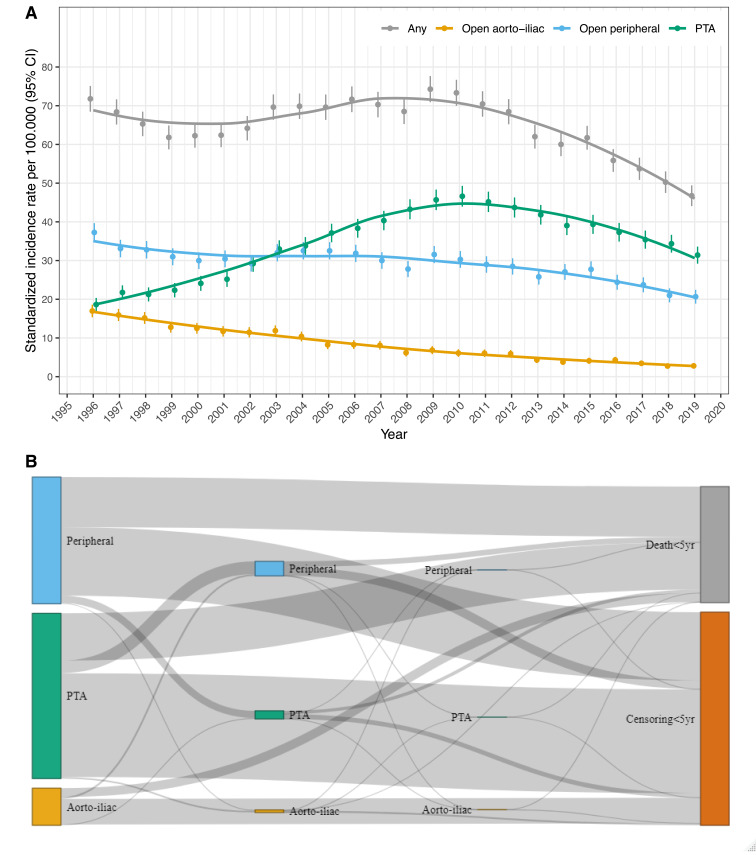
Results: We identified 41,438 unique patients undergoing 46,236 incident first-time LEAD repairs by either aorto-iliac- (n=5213), peripheral surgery (n=18,665) or percutaneous transluminal angioplasty (PTA, n=22,358). From 1996 to 2018, the age- and sex-standardized IR for primary revascularization declined from 71.8 to 50.2 per 100,000 person-years (IRR, 0.70; 95% CI, 0.66-0.75). Following a 2.5-fold IR increase of PTA from 1996 to 2010, all three repair techniques showed a declining trend after 2010. The declining IR was driven by decreasing LEAD repair due to claudication, and by persons aged below 80 years, while the IR increased in persons aged above 80 years (p interaction<0.001). LEAD repair was more frequent in men (IRRfemale vs male, 0.78; 95% CI, 0.77-0.80), which was consistent over calendar time (p interaction=0.41). Crude mortality decreased following open/surgical repair, and increased following PTA, but all three techniques trended towards lower adjusted mortality comparing the start and the end of the study period (MRRaorto-iliac, 0.71; 95% CI, 0.54-0.93 vs MRRperipheral, 0.76; 95% CI, 0.69-0.83 vs MRRPTA, 0.96; 95% CI, 0.86-1.07). Increasing age and CCI, male sex, smoking, and care dependency associated with increased mortality.
Conclusion: The incidence rate of LEAD repair decreased in Denmark from 1996 to 2018, especially in persons younger than 80 years, and primarily due to reduced revascularization for claudication. Adjusted mortality rates decreased following open surgery, but seemed unaltered following PTA.
Keywords: Danish National Patient Registry; Danish Vascular Registry; claudication; critical limb ischemia; registers; vascular surgery.
© 2024 Møller et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures




References
-
- Aboyans V, Ricco JB, Bartelink MEL, et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: the European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur Heart J. 2018;39(9):763–816. doi: 10.1093/eurheartj/ehx095 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
