Influencing factors of futile recanalization after endovascular intervention in patients with acute basilar artery occlusion
- PMID: 38501295
- PMCID: PMC11057989
- DOI: 10.3724/zdxbyxb-2023-0425
Influencing factors of futile recanalization after endovascular intervention in patients with acute basilar artery occlusion
Abstract
Objectives: To explore the influence factors for futile recanalization following endovascular treatment (EVT) in patients with acute basilar artery occlusion (BAO).
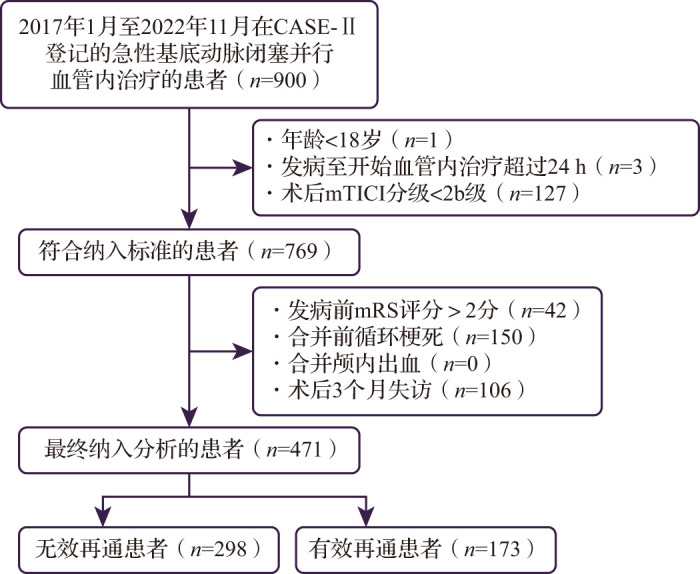
Methods: Clinical data of patients with acute BAO, who underwent endovascular treatment within 24 h of onset from January 2017 to November 2022, were retrospectively analyzed. The futile recanalization was defined as modified thrombolysis in cerebral infarction (mTICI) grade ≥2b or 3 after successful reperfusion, but the modified Rankin Scale score >2 at 3 months after EVT. Binary logistic regression model was used to analyze the influencing factors of futile recanalization.
Results: A total of 471 patients with a median age of 68 (57, 74) years were included and 68.9% were males, among whom 298 (63.27%) experienced futile recanalization. Multivariate analysis revealed that concomitant atrial fibrillation (OR=0.456, 95%CI: 0.282-0.737, P<0.01), bridging thrombolysis (OR=0.640, 95%CI: 0.416-0.985, P<0.05), achieving mTICI grade 3 (OR=0.554, 95%CI: 0.334-0.918, P<0.05), arterial occlusive lesion (AOL) grade 3 (OR=0.521, 95%CI: 0.326-0.834, P<0.01), and early postoperative statin therapy (OR=0.509, 95%CI: 0.273-0.948, P<0.05) were protective factors for futile recanalization after EVT in acute BAO patients. High baseline National Institutes of Health Stroke Scale (NIHSS) score (OR=1.068, 95%CI: 1.049-1.087, P<0.01), coexisting hypertension (OR=1.571, 95%CI: 1.017-2.427, P<0.05), multiple retrieval attempts (OR=1.237, 95%CI: 1.029-1.488, P<0.05) and postoperative hemorrhagic transformation (OR=8.497, 95%CI: 2.879-25.076, P<0.01) were risk factors. For trial of ORG 10172 in acute stroke treatment (TOAST) classification, cardiogenic embolism (OR=0.321, 95%CI: 0.193-0.534, P<0.01) and other types (OR=0.499, 95%CI: 0.260-0.961, P<0.05) were related to lower incidence of futile recanalization.
Conclusions: The incidence of futile recanalization after EVT in patients with acute BAO is high. Bridging venous thrombolysis before operation and an early postoperative statin therapy may reduce the incidence of futile recanalization.
目的: 探索急性基底动脉闭塞患者接受血管内治疗后发生无效再通的影响因素。方法: 对2017年1月至2022年11月影像学证实为急性基底动脉闭塞并在发病24 h内行血管内治疗的急性缺血性脑卒中患者的临床资料(来源于CASE-Ⅱ研究,NCT04487340)进行回顾性分析。以血管内治疗后改良脑梗死溶栓(mTICI)分级为2b级或3级,但3个月改良Rankin量表评分超过2分为无效再通,采用二元logistic回归模型分析发生无效再通的影响因素。结果: 共纳入患者471例,平均年龄为68(57,74)岁,男性占比为68.9%,其中298(63.27%)例发生了无效再通。多因素分析显示,急性基底动脉闭塞血管内治疗无效再通的保护性因素包括合并心房颤动(OR=0.456,95%CI:0.282~0.737,P<0.01)、桥接静脉溶栓(OR=0.640,95%CI:0.416~0.985,P<0.05)、mTICI分级3级(OR=0.554,95%CI:0.334~0.918,P<0.05)、动脉闭塞性病变分级3级(OR=0.521,95%CI:0.326~0.834,P<0.01)、术后早期他汀类药物治疗(OR=0.509,95%CI:0.273~0.948,P<0.05);而危险性因素包括基线美国国立卫生院卒中量表评分高(OR=1.068,95%CI:1.049~1.087,P<0.01)、合并高血压病(OR=1.571,95%CI:1.017~2.427,P<0.05)、取栓次数多(OR=1.237,95%CI:1.029~1.488,P<0.05)、术后24 h发生出血转化(OR=8.497,95%CI:2.879~25.076,P<0.01)。此外,心源性栓塞(OR=0.321,95%CI:0.193~0.534,P<0.01)和其他类型ORG 10172急性脑卒中治疗分类试验(TOAST)分型(OR=0.499,95%CI:0.260~0.961,P<0.05)与发生更低比例的无效再通相关。结论: 急性基底动脉闭塞患者接受血管内治疗后发生无效再通比例高,血管内治疗前桥接静脉溶栓和术后早期应用他汀类药可能可以降低无效再通的发生率。.
Keywords: Acute ischemic stroke; Basilar artery; Endovascular treatment; Recanalization; Retrospetive study.
Conflict of interest statement
所有作者均声明不存在利益冲突
The authors declare that there is no conflict of interests
Similar articles
-
[Influencing factors of futile recanalization after endovascular therapy in acute ischemic stroke patients with large vessel occlusions].Zhonghua Yi Xue Za Zhi. 2023 Aug 8;103(29):2218-2224. doi: 10.3760/cma.j.cn112137-20230218-00231. Zhonghua Yi Xue Za Zhi. 2023. PMID: 37544757 Chinese.
-
Futile Recanalization After Endovascular Treatment in Patients With Acute Basilar Artery Occlusion.Neurosurgery. 2023 May 1;92(5):1006-1012. doi: 10.1227/neu.0000000000002313. Epub 2022 Dec 29. Neurosurgery. 2023. PMID: 36700757
-
[The association between cortical venous outflow and futile recanalization in patients with acute ischemic stroke due to large vessel occlusion in the anterior circulation].Zhonghua Yi Xue Za Zhi. 2023 Aug 8;103(29):2210-2217. doi: 10.3760/cma.j.cn112137-20221230-02729. Zhonghua Yi Xue Za Zhi. 2023. PMID: 37544756 Chinese.
-
Endovascular Thrombectomy for Acute Basilar Artery Occlusion: Latest Findings and Critical Thinking on Future Study Design.Transl Stroke Res. 2022 Dec;13(6):913-922. doi: 10.1007/s12975-022-01008-5. Epub 2022 Mar 29. Transl Stroke Res. 2022. PMID: 35349051 Free PMC article. Review.
-
Endovascular thrombectomy with or without intravenous thrombolysis in acute basilar artery occlusion ischemic stroke: A meta-analysis.J Stroke Cerebrovasc Dis. 2022 Dec;31(12):106847. doi: 10.1016/j.jstrokecerebrovasdis.2022.106847. Epub 2022 Oct 28. J Stroke Cerebrovasc Dis. 2022. PMID: 36323166
References
-
- LANGEZAAL L, VAN DER HOEVEN E, MONT’ALVERNE F, et al. . Endovascular therapy for stroke due to basilar-artery occlusion[J]. N Engl J Med, 2021, 384(20): 1910-1920. - PubMed
-
- MEINEL T R, KAESMACHER J, CHALOULOS-IAKOVIDIS P, et al. . Mechanical thrombectomy for basilar artery occlusion: efficacy, outcomes, and futile recanalization in comparison with the anterior circulation[J]. J Neurointerv Surg, 2019, 11(12): 1174-1180. 10.1136/neurintsurg-2018-014516 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources