

A direct spinal cord-computer interface enables the control of the paralysed hand in spinal cord injury
- PMID: 38501612
- PMCID: PMC11449141
- DOI: 10.1093/brain/awae088
A direct spinal cord-computer interface enables the control of the paralysed hand in spinal cord injury
Abstract
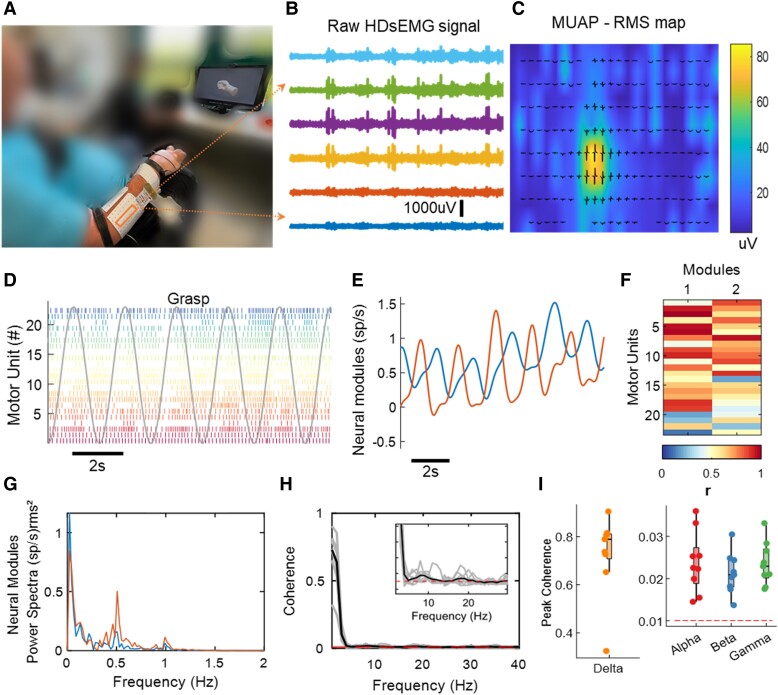
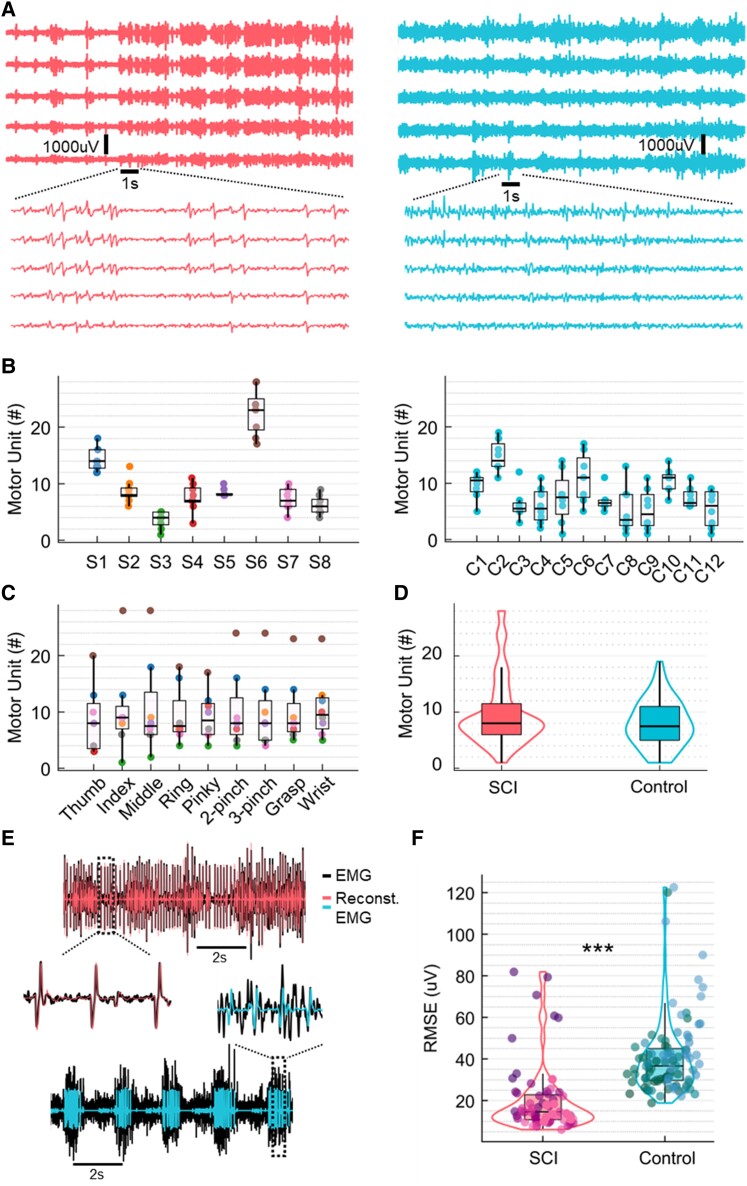
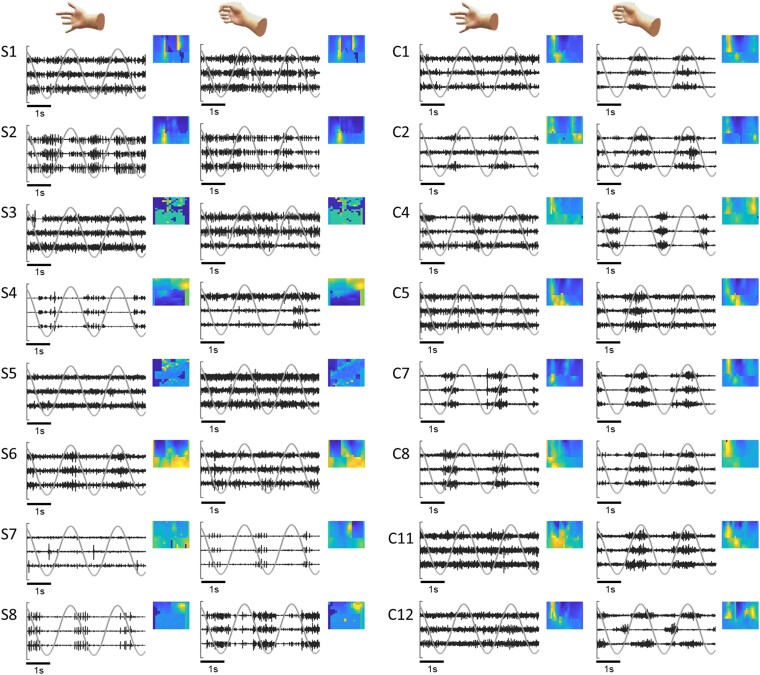
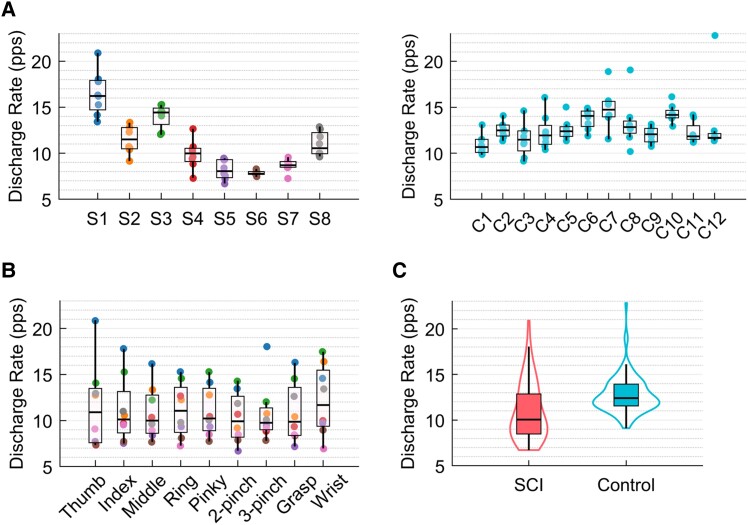
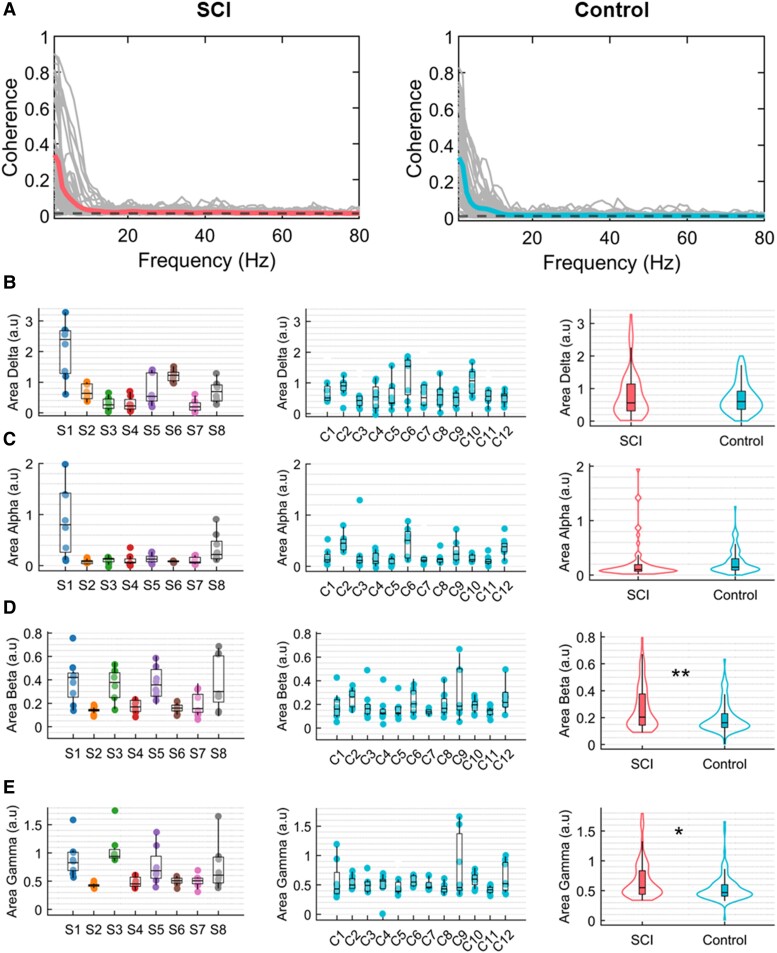
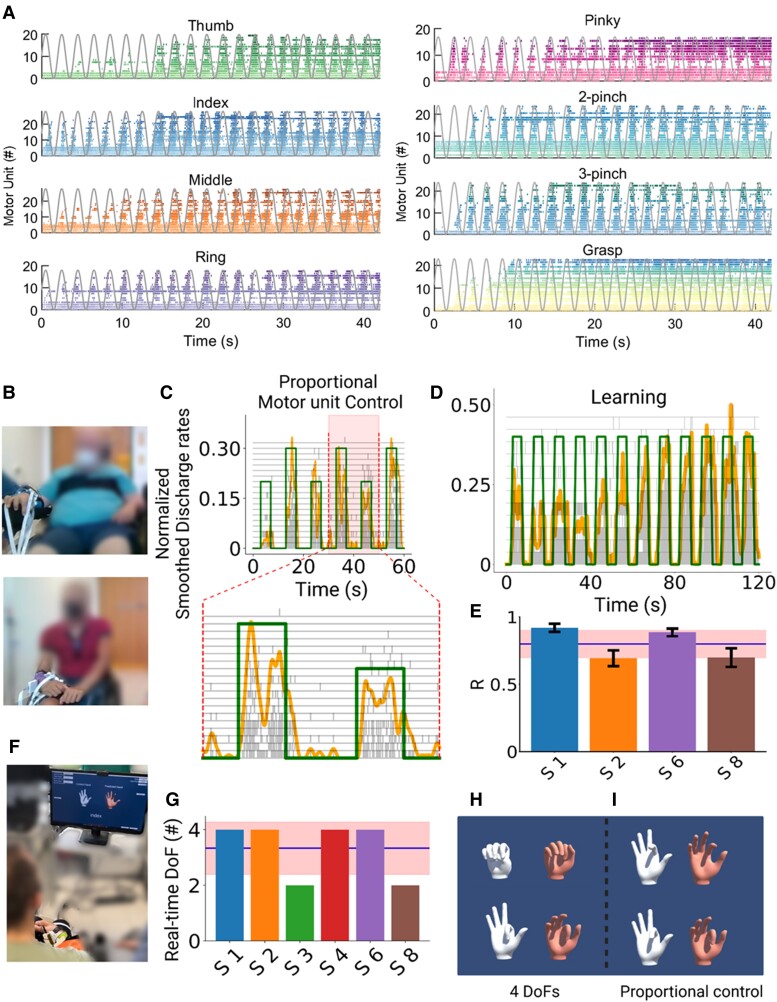
Paralysis of the muscles controlling the hand dramatically limits the quality of life for individuals living with spinal cord injury (SCI). Here, with a non-invasive neural interface, we demonstrate that eight motor complete SCI individuals (C5-C6) are still able to task-modulate in real-time the activity of populations of spinal motor neurons with residual neural pathways. In all SCI participants tested, we identified groups of motor units under voluntary control that encoded various hand movements. The motor unit discharges were mapped into more than 10 degrees of freedom, ranging from grasping to individual hand-digit flexion and extension. We then mapped the neural dynamics into a real-time controlled virtual hand. The SCI participants were able to match the cue hand posture by proportionally controlling four degrees of freedom (opening and closing the hand and index flexion/extension). These results demonstrate that wearable muscle sensors provide access to spared motor neurons that are fully under voluntary control in complete cervical SCI individuals. This non-invasive neural interface allows the investigation of motor neuron changes after the injury and has the potential to promote movement restoration when integrated with assistive devices.
Keywords: high density surface electromyography; motor neuron; motor unit; neural interface; spinal cord injury.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
The authors report no competing interests.
Figures
References
-
- Snoek GJ, Ijzerman MJ, Hermens HJ, Maxwell D, Biering-Sorensen F. Survey of the needs of patients with spinal cord injury: Impact and priority for improvement in hand function in tetraplegics. Spinal Cord. 2004;42:526–532. - PubMed
-
- Fridén J, House J, Keith M, Schibli S, van Zyl N. Improving hand function after spinal cord injury. J Hand Surg Eur. 2022;47:105–116. - PubMed
-
- Bouton CE, Shaikhouni A, Annetta NV, et al. Restoring cortical control of functional movement in a human with quadriplegia. Nature. 2016;533:247–250. - PubMed
-
- Benabid AL, Costecalde T, Eliseyev A, et al. An exoskeleton controlled by an epidural wireless brain–machine interface in a tetraplegic patient: A proof-of-concept demonstration. Lancet Neurol. 2019;18:1112–1122. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
