

Biomarkers Improve Diagnostics of Sepsis in Adult Patients With Suspected Organ Dysfunction Based on the Quick Sepsis-Related Organ Failure Assessment (qSOFA) Score in the Emergency Department
- PMID: 38502804
- PMCID: PMC11093432
- DOI: 10.1097/CCM.0000000000006216
Biomarkers Improve Diagnostics of Sepsis in Adult Patients With Suspected Organ Dysfunction Based on the Quick Sepsis-Related Organ Failure Assessment (qSOFA) Score in the Emergency Department
Abstract
Objectives: Consensus regarding biomarkers for detection of infection-related organ dysfunction in the emergency department is lacking. We aimed to identify and validate biomarkers that could improve risk prediction for overt or incipient organ dysfunction when added to quick Sepsis-related Organ Failure Assessment (qSOFA) as a screening tool.
Design: In a large prospective multicenter cohort of adult patients presenting to the emergency department with a qSOFA score greater than or equal to 1, admission plasma levels of C-reactive protein, procalcitonin, adrenomedullin (either bioavailable adrenomedullin or midregional fragment of proadrenomedullin), proenkephalin, and dipeptidyl peptidase 3 were assessed. Least absolute shrinkage and selection operator regression was applied to assess the impact of these biomarkers alone or in combination to detect the primary endpoint of prediction of sepsis within 96 hours of admission.
Setting: Three tertiary emergency departments at German University Hospitals (Jena University Hospital and two sites of the Charité University Hospital, Berlin).
Patients: One thousand four hundred seventy-seven adult patients presenting with suspected organ dysfunction based on qSOFA score greater than or equal to 1.
Interventions: None.
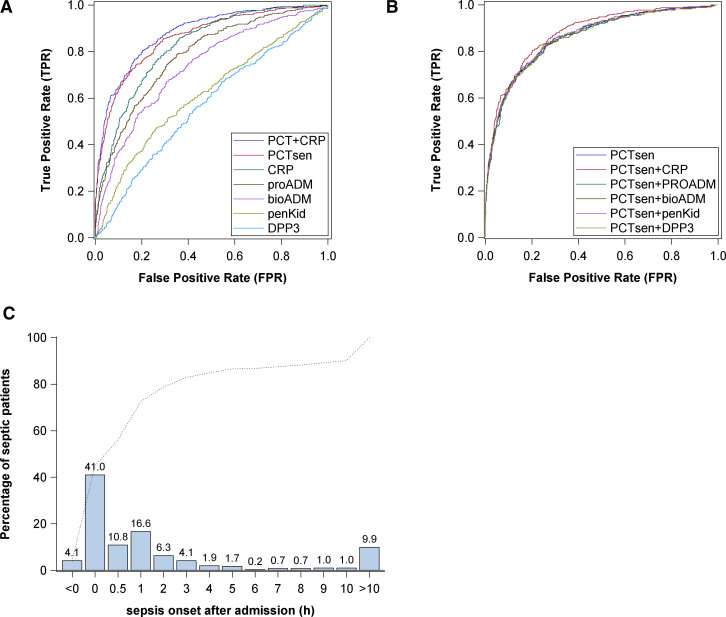
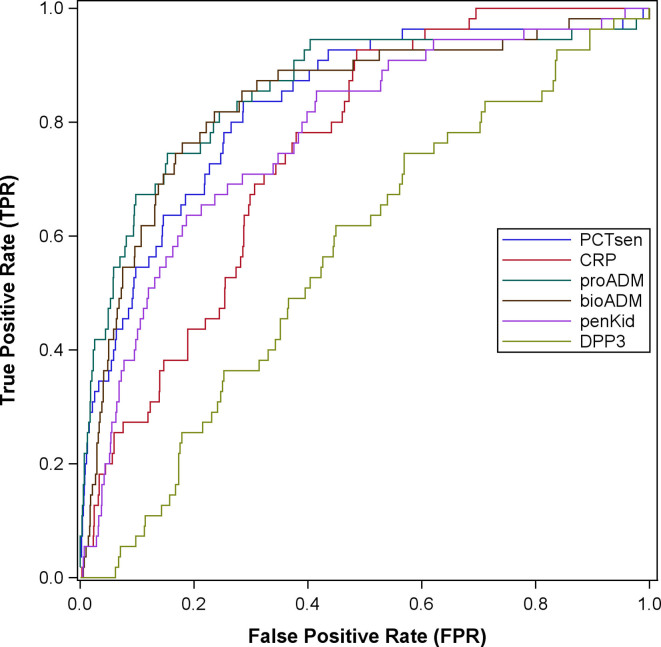
Measurements and main results: The cohort was of moderate severity with 81% presenting with qSOFA = 1; 29.2% of these patients developed sepsis. Procalcitonin outperformed all other biomarkers regarding the primary endpoint (area under the curve for receiver operating characteristic [AUC-ROC], 0.86 [0.79-0.93]). Adding other biomarkers failed to further improve the AUC-ROC for the primary endpoint; however, they improved the model regarding several secondary endpoints, such as mortality, need for vasopressors, or dialysis. Addition of procalcitonin with a cutoff level of 0.25 ng/mL improved net (re)classification by 35.2% compared with qSOFA alone, with positive and negative predictive values of 60.7% and 88.7%, respectively.
Conclusions: Biomarkers of infection and organ dysfunction, most notably procalcitonin, substantially improve early prediction of sepsis with added value to qSOFA alone as a simple screening tool on emergency department admission.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine and Wolters Kluwer Health, Inc.
Conflict of interest statement
Drs. Bolanaki’s, Winning’s, Slagman’s, Kiehntopf’s, Stacke’s, and Möckel’s institutions received funding from the Federal Ministry of Education and Research (Germany) (Bundesministerium für Bildung und Forschung [BMBF]). Dr. Slagman reports research funds from the German Research Council (Deutsche Forschungsgemeinschaft), the Innovation Fonds (Gemeinsamer Bundesausschuss), Roche Diagnostics, and ThermoFisher BRAHMS. Dr. Bolanaki reports funds from the Roche Diagnostics and ThermoFisher BRAHMS. Dr. Reinhart reported research grants from the Innovation Fonds (Gemeinsamer Bundesausschuss) and holds shares of the InflaRx NV, Jena, Germany. Dr. Bauer participated in advisory boards of BRAHMS/ThermoFisher and Roche Diagnostics regarding the use of biomarkers to diagnose sepsis. Dr. Winning disclosed he is an employee of the Jena University Hospital (JUH) and at the Ernst-Abbe-Hochschule in Jena. Drs. Kiehntopf’s and Bauer’s institutions received funding from the BMBF (Grant No. 03ZZ0810B). Dr. Kiehntopf disclosed they are inventor of a patent covering a method for quantification of C-terminal peptides of α1-antitrypsin (applicant: JUH; EP22154836.5; status: application), and the inventor of other patents covering C-terminal AAT peptides in inflammation (applicant: JUH: Method for determining the origin of an infection; EP17719610.2 [application]; EP3239712 [granted]) and Diagnosis of Sepsis and Systemic Inflammatory Response Syndrome (CN104204808B, EP2592421, EP2780719, US10712350B2, JP6308946B2 [all granted]). Dr. Möckel’s institution received funding from Roche Molecular Diagnostics German Innovation Funds; he received funding from ThermoFisher BRAHMS GmbH, AstraZeneca, Abbott, Medtronic, Radiometer, and Sanofi; and he disclosed he is Editor-in-Chief of Biomarkers. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures

Comment in
-
Can Procalcitonin and Other Biomarkers Help Rapidly Identify Sepsis Among Undifferentiated High-Risk Patients in the Emergency Department?Crit Care Med. 2024 Jun 1;52(6):979-982. doi: 10.1097/CCM.0000000000006241. Epub 2024 May 16. Crit Care Med. 2024. PMID: 38752815 No abstract available.
References
-
- Singer M, Inada-Kim M, Shankar-Hari M: Sepsis hysteria: Excess hype and unrealistic expectations. Lancet. 2019; 394:1513–1514 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
