

NMR and MS reveal characteristic metabolome atlas and optimize esophageal squamous cell carcinoma early detection
- PMID: 38504100
- PMCID: PMC10951220
- DOI: 10.1038/s41467-024-46837-0
NMR and MS reveal characteristic metabolome atlas and optimize esophageal squamous cell carcinoma early detection
Abstract
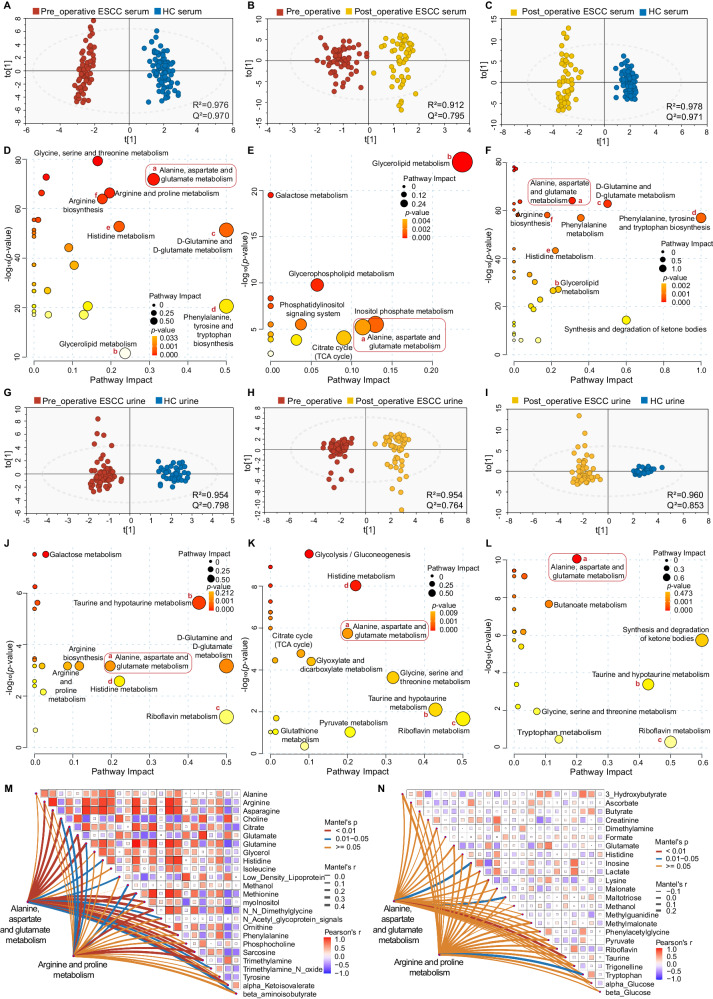
Metabolic changes precede malignant histology. However, it remains unclear whether detectable characteristic metabolome exists in esophageal squamous cell carcinoma (ESCC) tissues and biofluids for early diagnosis. Here, we conduct NMR- and MS-based metabolomics on 1,153 matched ESCC tissues, normal mucosae, pre- and one-week post-operative sera and urines from 560 participants across three hospitals, with machine learning and WGCNA. Aberrations in 'alanine, aspartate and glutamate metabolism' proved to be prevalent throughout the ESCC evolution, consistently identified by NMR and MS, and reflected in 16 serum and 10 urine metabolic signatures in both discovery and validation sets. NMR-based simplified panels of any five serum or urine metabolites outperform clinical serological tumor markers (AUC = 0.984 and 0.930, respectively), and are effective in distinguishing early-stage ESCC in test set (serum accuracy = 0.994, urine accuracy = 0.879). Collectively, NMR-based biofluid screening can reveal characteristic metabolic events of ESCC and be feasible for early detection (ChiCTR2300073613).
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures






Similar articles
-
A multi-platform metabolomics reveals possible biomarkers for the early-stage esophageal squamous cell carcinoma.Anal Chim Acta. 2022 Aug 8;1220:340038. doi: 10.1016/j.aca.2022.340038. Epub 2022 Jun 8. Anal Chim Acta. 2022. PMID: 35868700
-
Integrating transcriptome and metabolome variability to reveal pathogenesis of esophageal squamous cell carcinoma.Biochim Biophys Acta Mol Basis Dis. 2021 Jan 1;1867(1):165966. doi: 10.1016/j.bbadis.2020.165966. Epub 2020 Sep 12. Biochim Biophys Acta Mol Basis Dis. 2021. PMID: 32931889
-
Towards Tyrosine Metabolism in Esophageal Squamous Cell Carcinoma.Comb Chem High Throughput Screen. 2017;20(2):133-139. doi: 10.2174/1386207319666161220115409. Comb Chem High Throughput Screen. 2017. PMID: 28000565
-
Untargeted metabolomics analysis of esophageal squamous cell cancer progression.J Transl Med. 2022 Mar 14;20(1):127. doi: 10.1186/s12967-022-03311-z. J Transl Med. 2022. PMID: 35287685 Free PMC article. Review.
-
Molecular alterations and clinical relevance in esophageal squamous cell carcinoma.Front Med. 2013 Dec;7(4):401-10. doi: 10.1007/s11684-013-0286-y. Epub 2013 Sep 3. Front Med. 2013. PMID: 24002746 Review.
Cited by
-
From multi-omics to predictive biomarker: AI in tumor microenvironment.Front Immunol. 2024 Dec 23;15:1514977. doi: 10.3389/fimmu.2024.1514977. eCollection 2024. Front Immunol. 2024. PMID: 39763649 Free PMC article. Review.
-
NMR-based metabolomics combined with metabolic pathway analysis reveals metabolic heterogeneity of colorectal cancer tissue at different anatomical locations and stages.Int J Cancer. 2025 Apr 15;156(8):1644-1655. doi: 10.1002/ijc.35273. Epub 2024 Dec 4. Int J Cancer. 2025. PMID: 39629979 Free PMC article.
-
A metabolomic profile of biological aging in 250,341 individuals from the UK Biobank.Nat Commun. 2024 Sep 15;15(1):8081. doi: 10.1038/s41467-024-52310-9. Nat Commun. 2024. PMID: 39278973 Free PMC article.
-
Pluripotent stem cell-derived extracellular vesicles for systemic immune modulation in diabetes therapy.Res Sq [Preprint]. 2025 Jun 10:rs.3.rs-6415252. doi: 10.21203/rs.3.rs-6415252/v1. Res Sq. 2025. PMID: 40585231 Free PMC article. Preprint.
-
Elucidating the Mechanisms of Acquired Palbociclib Resistance via Comprehensive Metabolomics Profiling.Curr Issues Mol Biol. 2025 Jan 2;47(1):24. doi: 10.3390/cimb47010024. Curr Issues Mol Biol. 2025. PMID: 39852139 Free PMC article.
References
-
- Wang, Y. et al. Global burden of digestive diseases: a systematic analysis of the global burden of diseases study, 1990 to 2019. Gastroenterology. 10.1053/j.gastro.2023.05.050 (2023). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
