

A meta-analysis and trial sequential analysis of randomised controlled trials comparing nonoperative and operative management of chest trauma with multiple rib fractures
- PMID: 38504282
- PMCID: PMC10949653
- DOI: 10.1186/s13017-024-00540-z
A meta-analysis and trial sequential analysis of randomised controlled trials comparing nonoperative and operative management of chest trauma with multiple rib fractures
Abstract
Background: Operative treatment of traumatic rib fractures for better outcomes remains under debate. Surgical stabilization of rib fractures has dramatically increased in the last decade. This study aimed to perform a systematic review and meta-analysis of randomised controlled trials (RCTs) to assess the effectiveness and safety of operative treatment compared to conservative treatment in adult patients with traumatic multiple rib fractures.
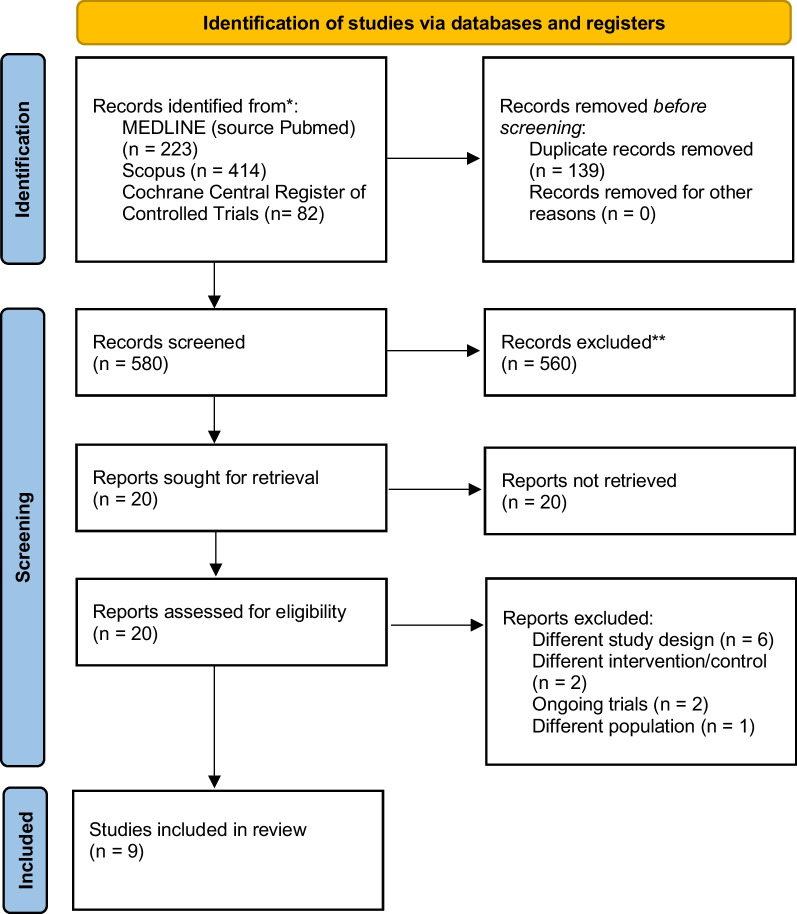
Methods: A systematic literature review was performed according to the preferred reporting items for systematic reviews and meta-analyses guidelines. We searched MEDLINE, Scopus, and Cochrane Central Register of Controlled Trials and used the Cochrane Risk-of-Bias 2 tool to evaluate methodological quality. Relative risks with 95% confidence interval (CI) were calculated for outcomes: all-cause mortality, pneumonia incidence, and number of mechanical ventilation days. Overall certainty of evidence was evaluated with the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach, with trial sequential analysis performed to establish implications for further research.
Results: From 719 records, we included nine RCTs, which recruited 862 patients. Patients were assigned to the operative group (received surgical stabilization of chest wall injury, n = 423) or control group (n = 439). All-cause mortality was not significantly different (RR = 0.53; 95% CI 0.21 to 1.38, P = 0.35, I2 = 11%) between the two groups. However, in the operative group, duration of mechanical ventilation (mean difference -4.62; 95% CI -7.64 to -1.60, P < 0.00001, I2 = 94%) and length of intensive care unit stay (mean difference -3.05; 95% CI -5.87 to -0.22; P < 0.00001, I2 = 96%) were significantly shorter, and pneumonia incidence (RR = 0.57; 95% CI 0.35 to 0.92; P = 0.02, I2 = 57%) was significantly lower. Trial sequential analysis for mortality indicated insufficient sample size for a definitive judgment. GRADE showed this meta-analysis to have very low to low confidence.
Conclusion: Meta-analysis of large-scale trials showed that surgical stabilization of multiple rib fractures shortened the duration of mechanical ventilation and reduced the incidence of pneumonia but lacked clear evidence for improvement of mortality compared to conservative treatment. Trial sequential analysis suggested the need for more cases, and GRADE highlighted low certainty, emphasizing the necessity for further targeted RCTs, especially in mechanically ventilated patients.
Systematic review registration: UMIN Clinical Trials Registry UMIN000049365.
Keywords: Chest trauma; Flail chest; Fracture stabilization; Rib fractures; Surgery fixation; Thoracic injury.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Haagsma JA, Graetz N, Bolliger I, Naghvi M, Higashi H, Mullany EC, et al. The global burden of injury: incidence, mortality, disability-adjusted life years and time trends from the global burden of disease study 2013. Inj Prev. 2016;22(1):3–18. doi: 10.1136/injuryprev-2015-041616. - DOI - PMC - PubMed
-
- Baghai M, Whitaker D. Thoracic trauma. In: Moorjani N, Viola N, Walker WS, (eds). Key Questions in Thoracic Surgery. 1st edition. Shrewsbury, UK: TFM Publishing Ltd.; 2016. P.971–988.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
